Clinical History:
- Past medical history: advanced esophageal adenocarcinoma status post radiation and chemo/immunotherapy with immune mediated hepatitis, and moderate alcohol use.
- Medications: nivolumab, FOLFOX chemotherapy (fluorouracil, folinic acid, and oxaliplatin), and prednisone.
- Physical exam: strength: bilateral mild proximal upper and severe lower extremity weakness; reflexes: silent in bilateral lower extremities; sensation decreased in feet and hands; no mandatory.
- Imaging: White matter volume loss and microvascular injury; no definite cord or neural foraminal compression.
- Lab results: highest CK 20,000 currently trending downward.
What agent is primarily responsible based on the reference images below?
A. Nivolumab
B. Fluorouracil
C. Oxaliplatin
D. Prednisone
Images for Reference:
Correct Answer:
Nivolumab – PD-1 / immune checkpoint inhibitor
Immune checkpoint inhibitor-associated myopathy (ICIAM)
- Primary differential diagnosis: immune mediated necrotizing myopathy (IMNM)
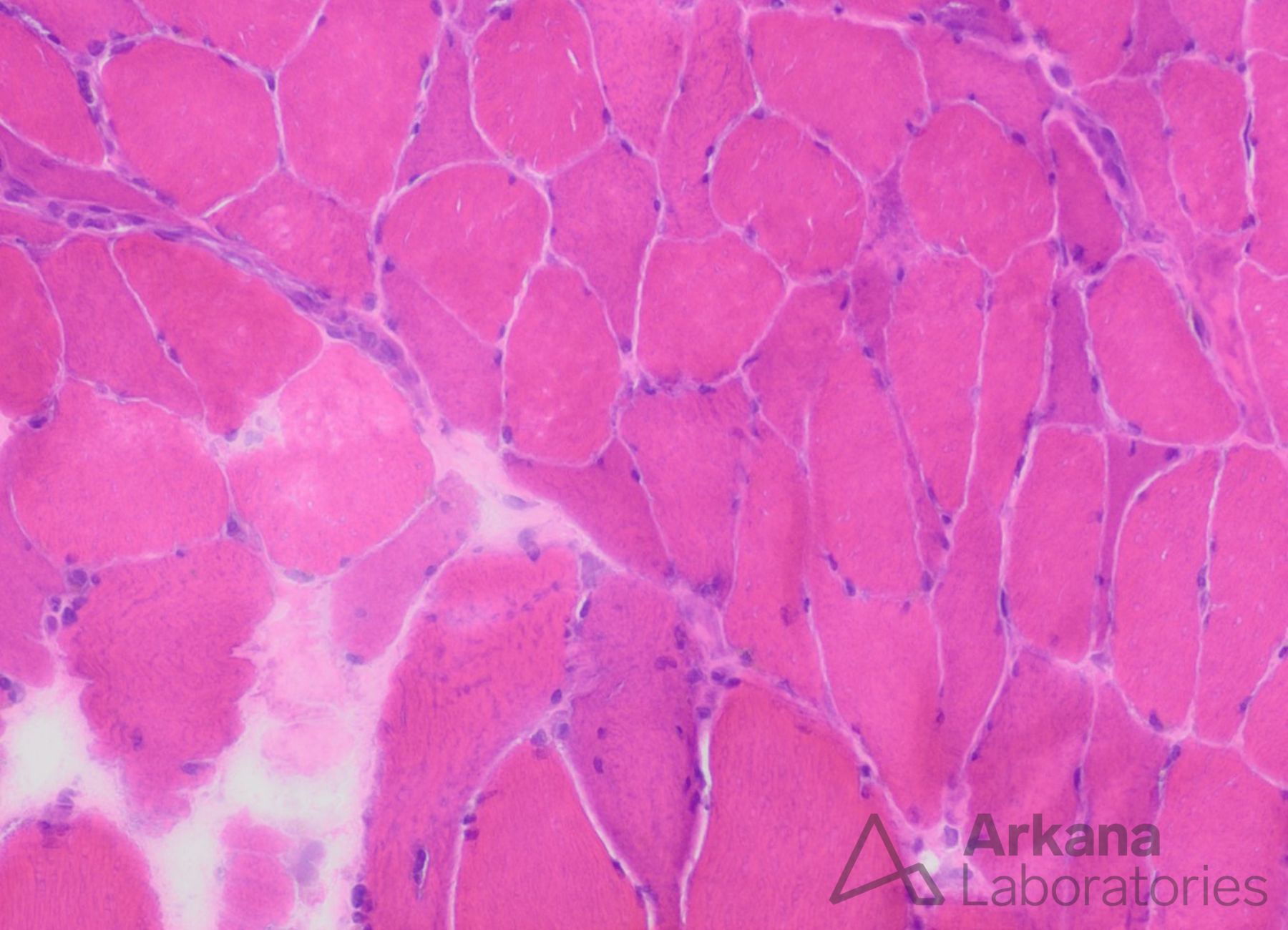
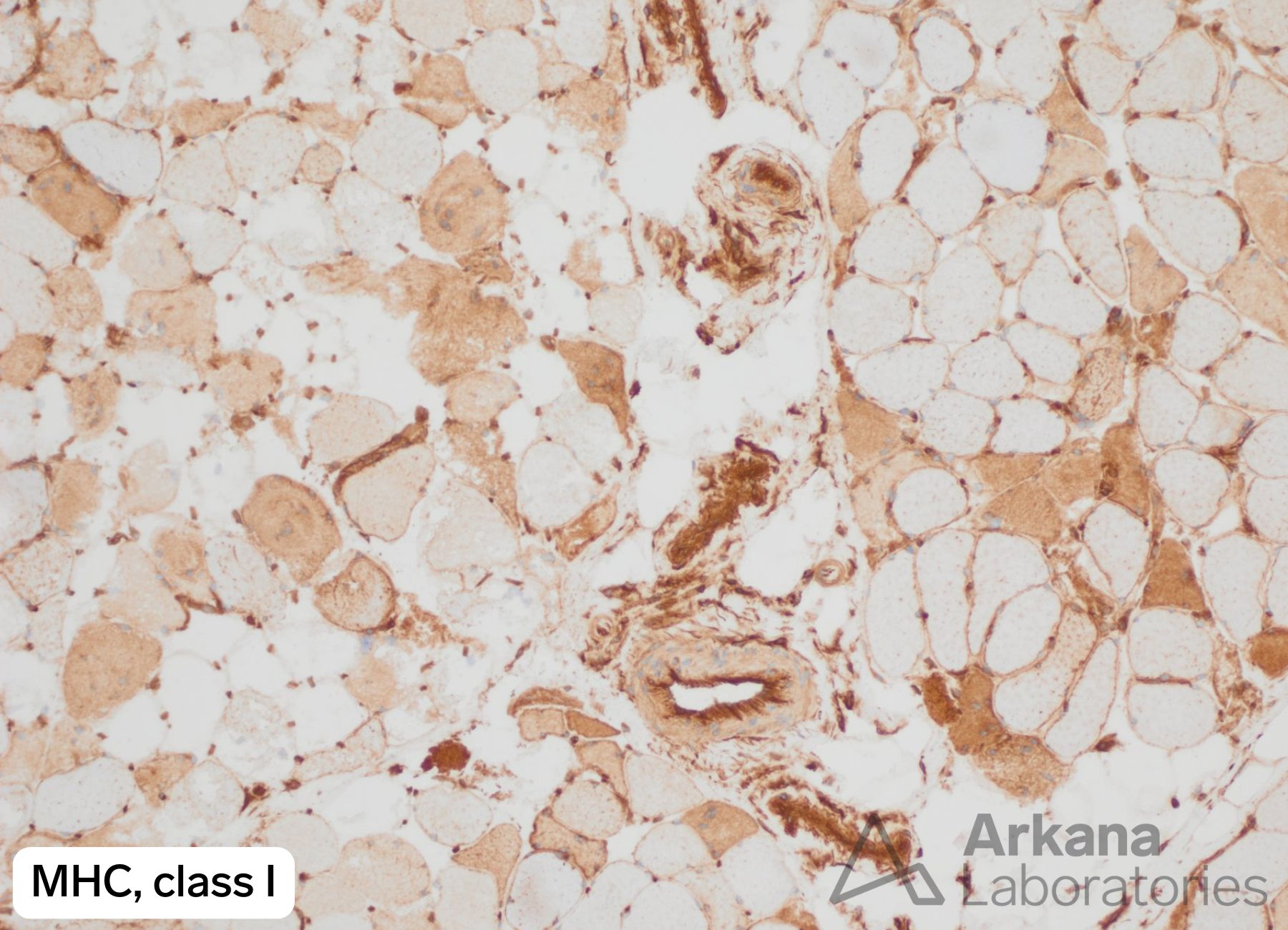
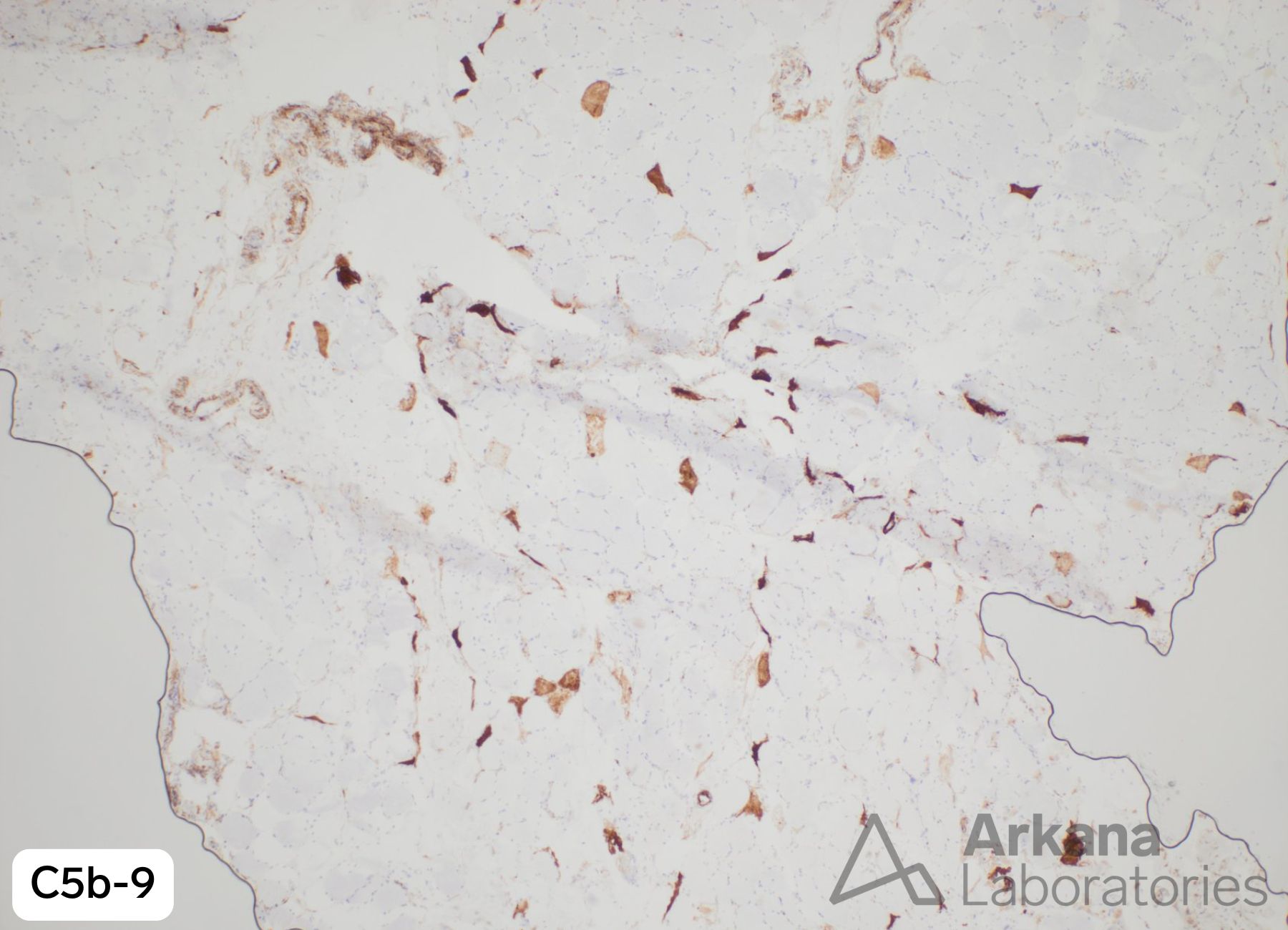
- Histologically:
- Multifocal clusters of necrotic cells
- Increased acid phosphatase reactivity in the connective tissue
- Less likely to have endomysial inflammation, invasion of non-necrotic fibers, vacuoles, internalized nuclei or fiber splitting than IMNM
- Both clinical and/or histological features of dermatomyositis have also been described in the setting of ICIAM.
Reference(s) / Additional Reading:
- Shelly S, Triplett JD, Pinto MV. Brain Commun. 2020;2:fcaa181.
- Guerra NL, et al. Autoimmun Rev. 2023;22:103375.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.