The patient is a middle-aged female (5th decade) who presents for hospital admission with severe progressive muscle weakness, failure to thrive, and fever of unknown origin, and developed respiratory failure requiring intubation with mechanical ventilation. Work-up revealed no definitive etiology or unifying diagnosis. Over the next two months her hospital course is complicated by cholangitis and cardiac arrest. Her past medical history is significant for polysubstance abuse. Physical exam notes quadriplegia and a subtle skin rash of the thighs, without other characteristic features. Muscle biopsy is pursued as she is unable to be weaned from the ventilator. Neuropathologic examination of the thigh muscle biopsy revealed changes most consistent with critical illness myopathy. Using the figures above, what are the cardinal neuropathologic features and findings of critical illness myopathy?
A. Correct Clinical Hx
B. Blue change on MGT
C. Loss of thick filaments
D. All of the above
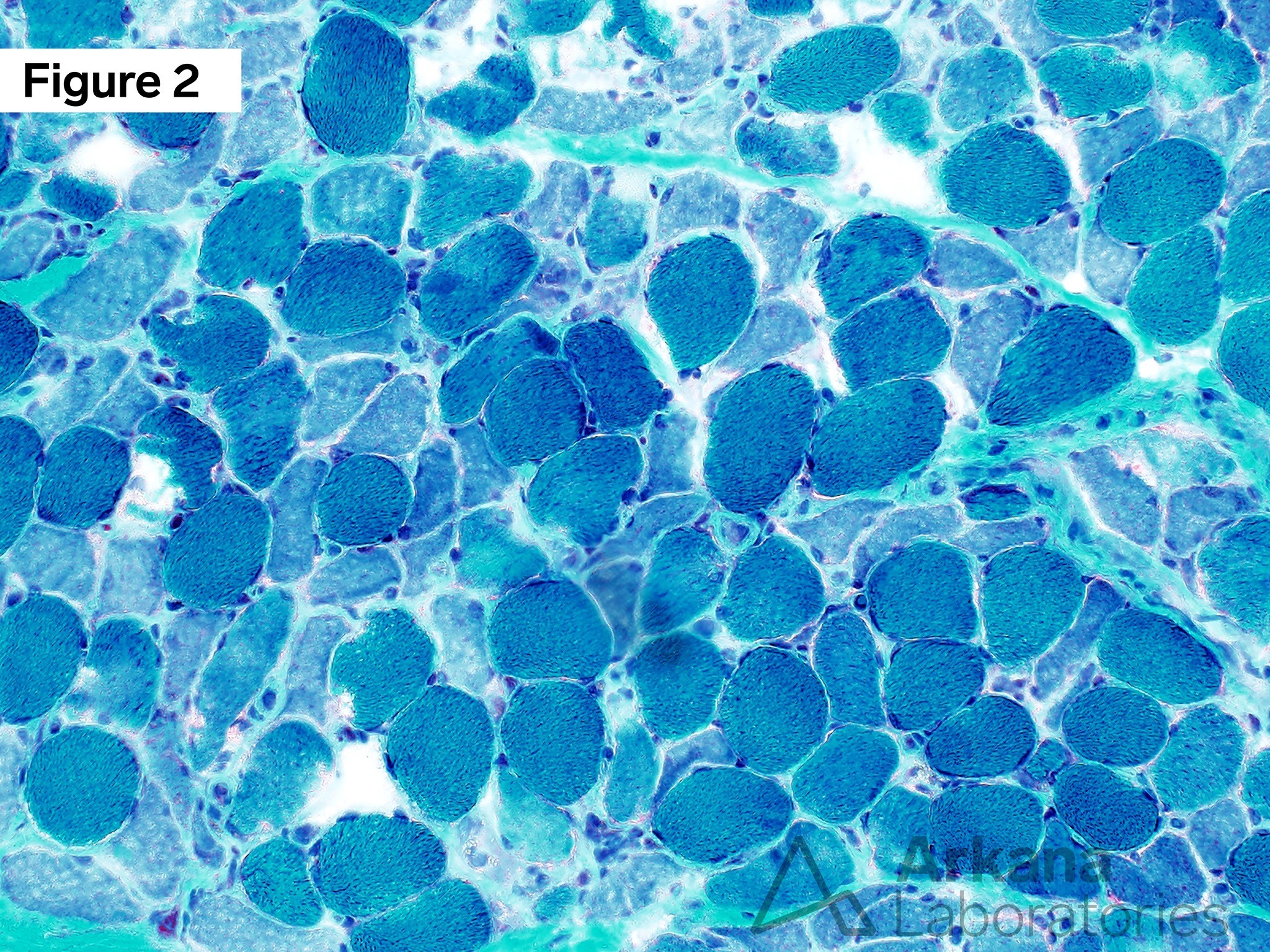
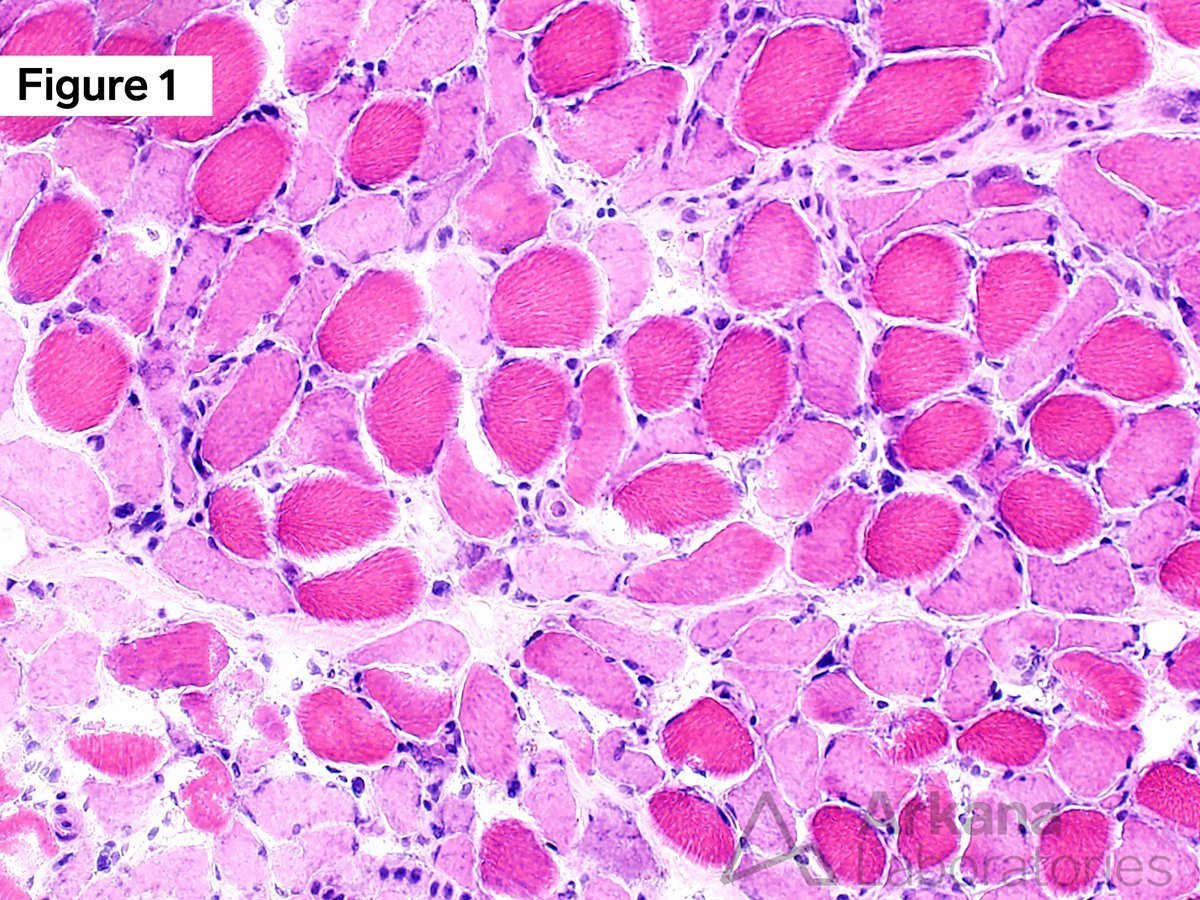
Skeletal muscle biopsy demonstrating changes of critical illness myopathy. (Figure 1) Hematoxylin and eosin (H&E)-stained section prepared from snap frozen skeletal muscle shows atrophic muscle with a subset of atrophic pale staining type 2 muscle fibers (fiber typing stains not shown), and relatively rare scattered mild nonspecific myopathic changes are seen through the specimen. (Figure 2) Muscle fibers have a blue tinctorial quality change on staining with Modified Gomori Trichrome (MGT).
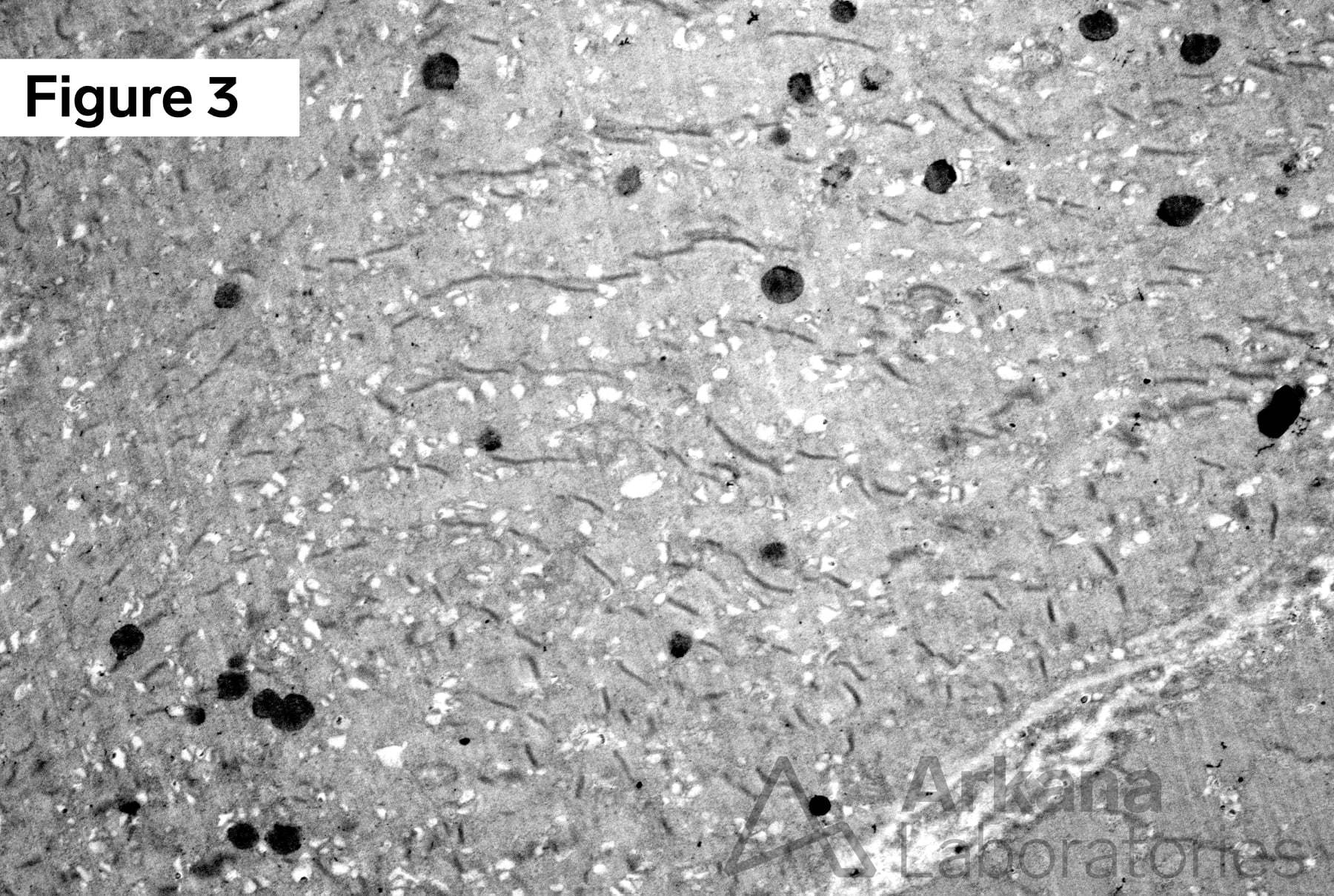
(Figure 3) Ultrastructural examination by electron microscopy (EM) shows loss of the myosin thick filaments and preservation of thin filaments and Z-lines. Original Magnifications: A. Frozen H&E, 100x; B. Frozen MGT, 100x; and C. EM, 2500x.
Answer: All of the above
If you chose answer choice (D) All the Above, then you got it! The neuropathologist must interpret the muscle biopsy findings with the clinical history in mind to provide the best possible integrative diagnosis, especially in medically complicated patients, as in this case. To learn more about critical illness myopathy (CIM), see the references below.
The salient features of critical illness myopathy are first and foremost that the proper clinical history be appropriate to consider critical illness myopathy. Of note, steroid-induced myopathy may also show similar features.
Next, standard muscle biopsy panel staining with Modified Gomori Trichrome (MGT) on frozen section material yields a blue (“blue-ish”) tinctorial quality change, as compared to otherwise normal green (“sea green” or “sea foam green”) staining of MGT.
Another essential finding in critical illness myopathy is loss of the myosin thick filaments (myosin heavy chain loss), which can be found by ultrastructural examination with electron microscopy (EM).
References
Friedrich O, Reid MB, Van den Berghe G, et al. The Sick and the Weak: Neuropathies/Myopathies in the Critically Ill. Physiol Rev. 2015 Jul;95(3):1025-109. PMID: 26133937.
Larsson L, Li X, Edström L, et al. Acute quadriplegia and loss of muscle myosin in patients treated with nondepolarizing neuromuscular blocking agents and corticosteroids: mechanisms at the cellular and molecular levels. Crit Care Med. 2000 Jan;28(1):34-45. PMID: 10667496.
Latronico N, Bolton CF. Critical illness polyneuropathy and myopathy: a major cause of muscle weakness and paralysis. Lancet Neurol. 2011 Oct;10(10):931-41. PMID: 21939902.
Shepherd S, Batra A, Lerner DP. Review of Critical Illness Myopathy and Neuropathy. Neurohospitalist. 2017 Jan;7(1):41-48. PMID: 28042370.
Z’Graggen WJ, Tankisi H. Critical Illness Myopathy. J Clin Neurophysiol. 2020 May;37(3):200-204. PMID: 32358245.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.