The patient is a 50-year-old male who presents with a chief complaint of generalized headaches. Neuroimaging reveals a 3.5 cm dural-based enhancing mass with a dural tail in the posterior fossa along the tentorium compressing the transverse sinus. Neurosurgery pursued suboccipital craniotomy and resection. Neuropathology showed a fibrous variant meningioma, WHO grade I. Using the images above, which of the following immunoprofiles best fits this brain tumor?
A. EMA+, SSTR2-, STAT6+
B. EMA+, SSTR2+, STAT6-
C. CD34+, SSTR2-, STAT6+
D. CD34+, SSTR2-, STAT6-
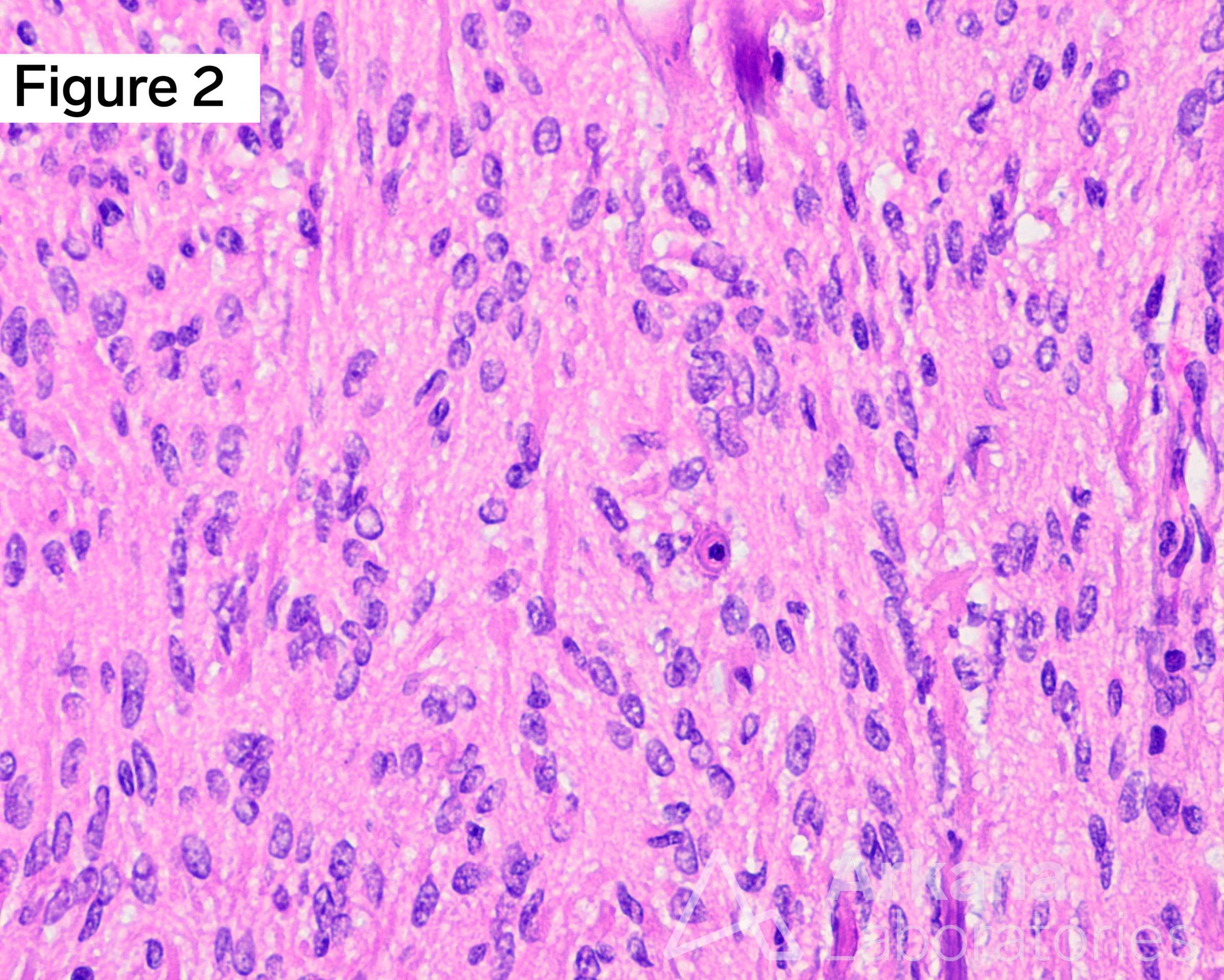
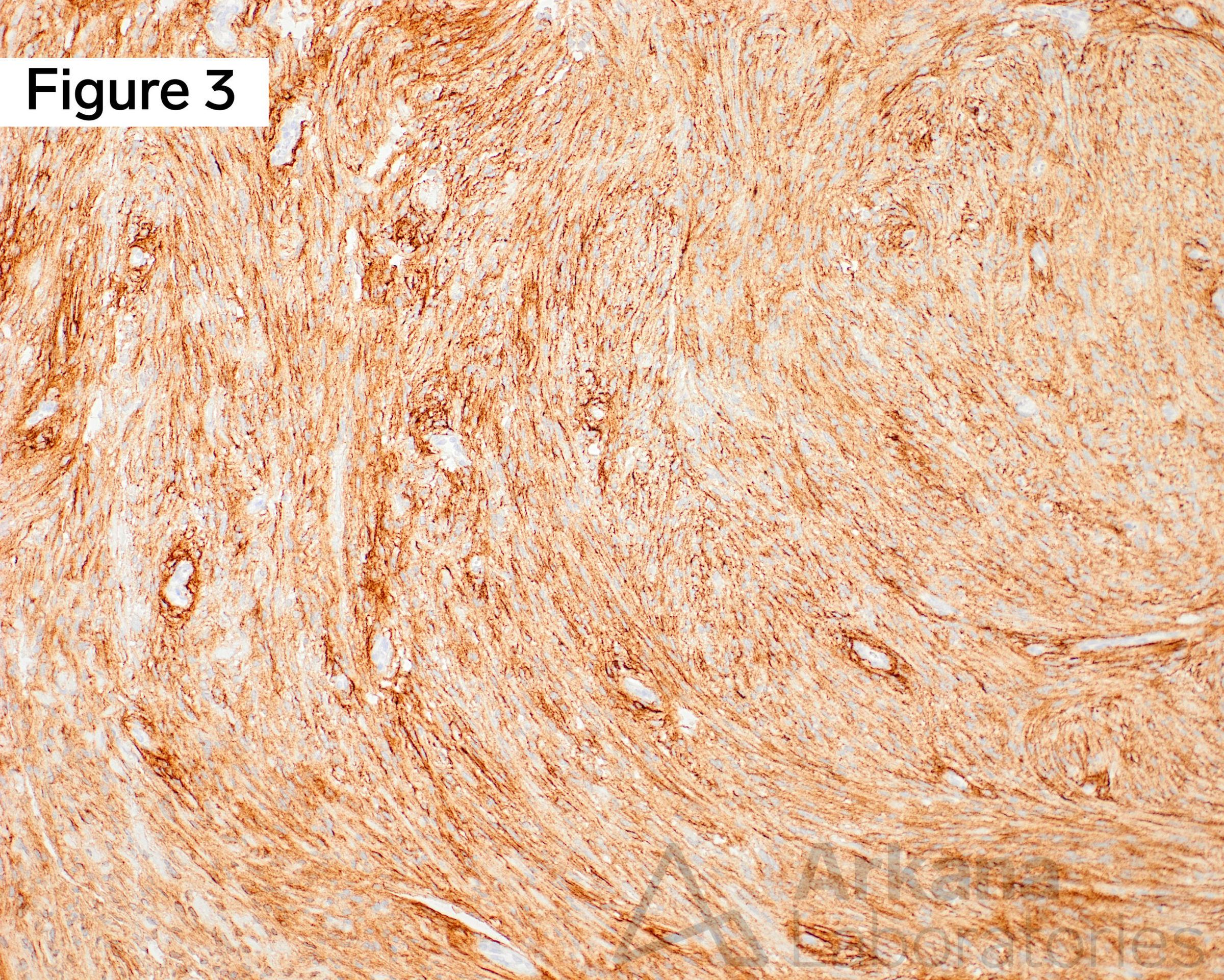
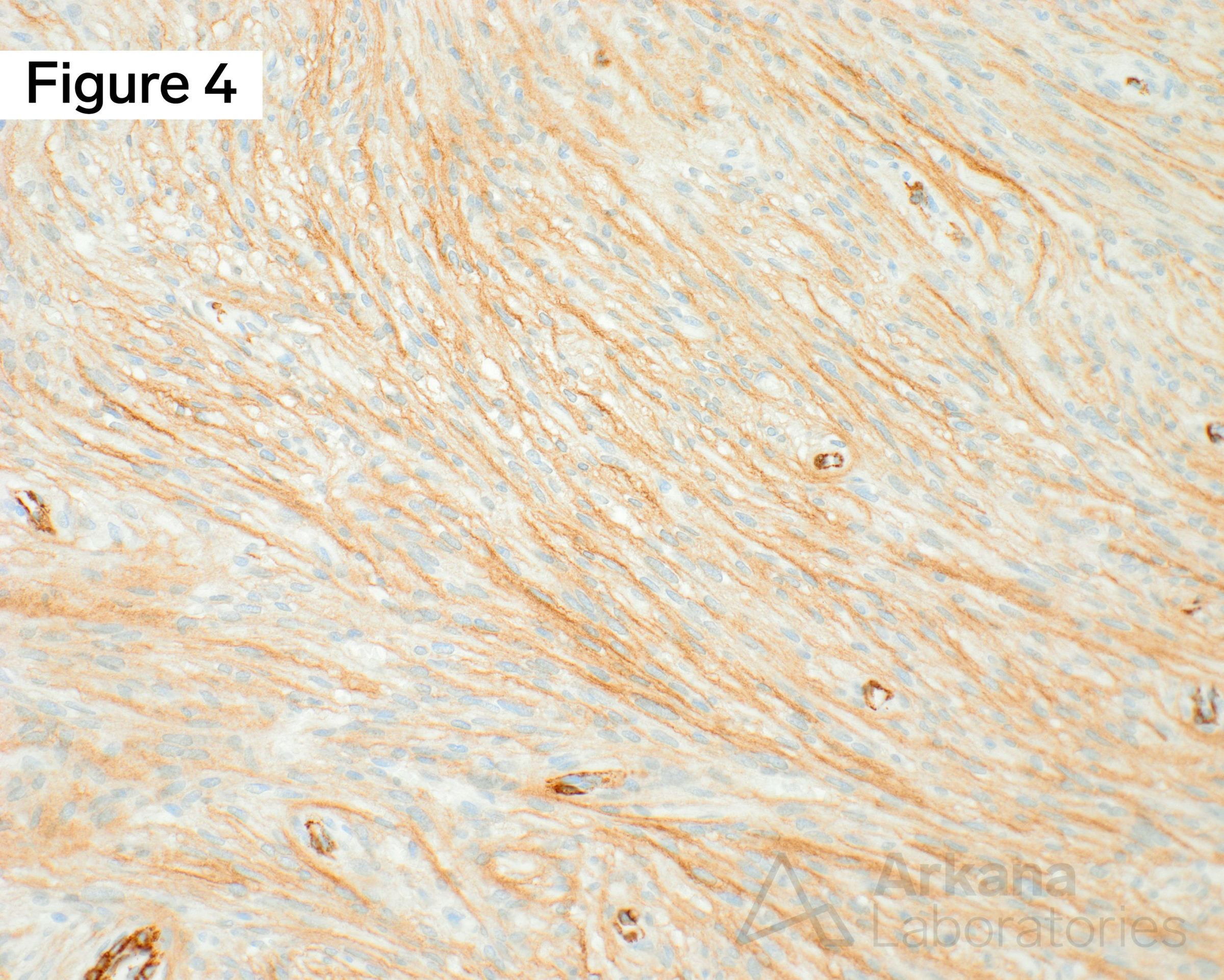
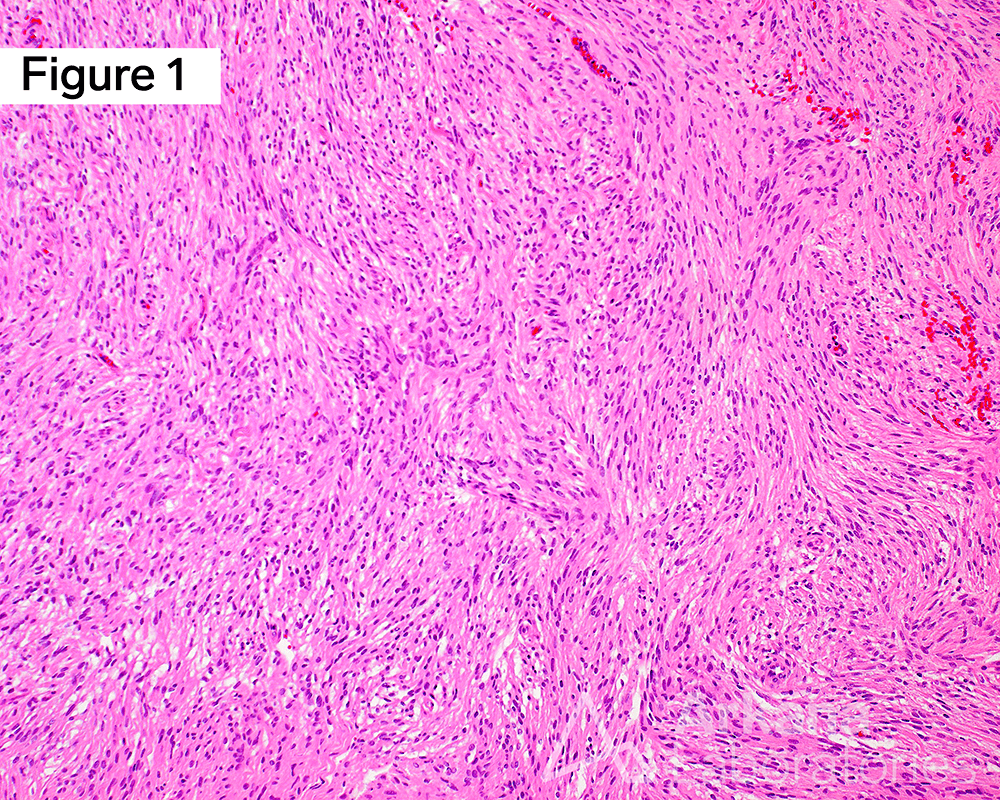
Immunoprofile of Meningioma, WHO grade I, Fibrous Variant. Hematoxylin and eosin (H&E)-stained sections show a dural-based spindle cell lesion arranged in broad sweeping fascicles without atypical features, higher grade growth patterns, or tumor necrosis (Figure 1), and at higher power there is an exceedingly rare mitotic figure, far less than 1 mitotic figure per 10 high-power fields (Figure 2). Immunohistochemical (IHC) work-up demonstrated strong diffuse membranous staining with epithelial membrane antigen (EMA+) (Figure 3), and positive immunoreactivity for somatostatin receptor 2A (SSTR2+) (Figure 4). Original magnifications: A. H&E, 100x; B. H&E, 400x; C. EMA, 100x; and D. SSTR2, 200x.
Answer: EMA+, SSTR2+, STAT6-
The brain tumor is a fibrous variant meningioma, WHO grade I, and while immunostaining is not always necessary for this diagnosis, there are diagnostic pitfalls that one ought to be mindful not to overlook.
The correct immunoprofile / immunophenotype for this meningioma is epithelial membrane antigen positive (EMA+), somatostatin receptor 2A positive (SSTR2+), and signal transducer and activator of transcription (STAT) 6 negative (STAT6-), answer choice (C).
The one common differential diagnosis list of spindle cell lesions of the dura might include meningioma, solitary fibrous tumor/hemangiopericytoma (SFT/HPC), schwannoma, neurofibroma, spindle cell melanoma, and synovial sarcoma, amongst other less common entities.
Why were the other answers wrong?
Each of the wrong answer choices could be an immunoprofile seen with solitary fibrous tumor / hemangiopericytoma (SFT/HPC), which are usually EMA+/-, CD34+, SSTR2A-, and STAT6+.
STAT6 is a highly sensitive and specific marker for SFT/HPC that is readily commercially available to any immunohistochemical (IHC) armamentarium.
If you come across a very rare SFT/HPC that is CD34+ and STAT6-, don’t give up, you may still be correct, but you may need to pursue molecular diagnostics to assay the characteristic NAB2-STAT6 fusion for integrated diagnosis.
References
Boulagnon-Rombi C, Fleury C, Fichel C, et al. Immunohistochemical Approach to the Differential Diagnosis of Meningiomas and Their Mimics. J Neuropathol Exp Neurol. 2017 Apr 1;76(4):289-298. PMID: 28340171.
Menke JR, Raleigh DR, Gown AM, et al. Somatostatin receptor 2a is a more sensitive diagnostic marker of meningioma than epithelial membrane antigen. Acta Neuropathol. 2015 Sep;130(3):441-3. PMID: 26195322.
Yoshida A, Tsuta K, Ohno M, Yet al. STAT6 immunohistochemistry is helpful in the diagnosis of solitary fibrous tumors. Am J Surg Pathol. 2014 Apr;38(4):552-9. PMID: 24625420.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.