Clinical History:
The 50-year-old patient was admitted for shortness of breath and acute muscle weakness following a viral illness. Laboratory studies showed elevated CPK (1200-1400 range) The patient was treated with steroid prior to muscle biopsy. No myotoxic medications were noted in the patient’s home medication list.
What is your pathologic diagnosis based on the reference images below?

Answer:
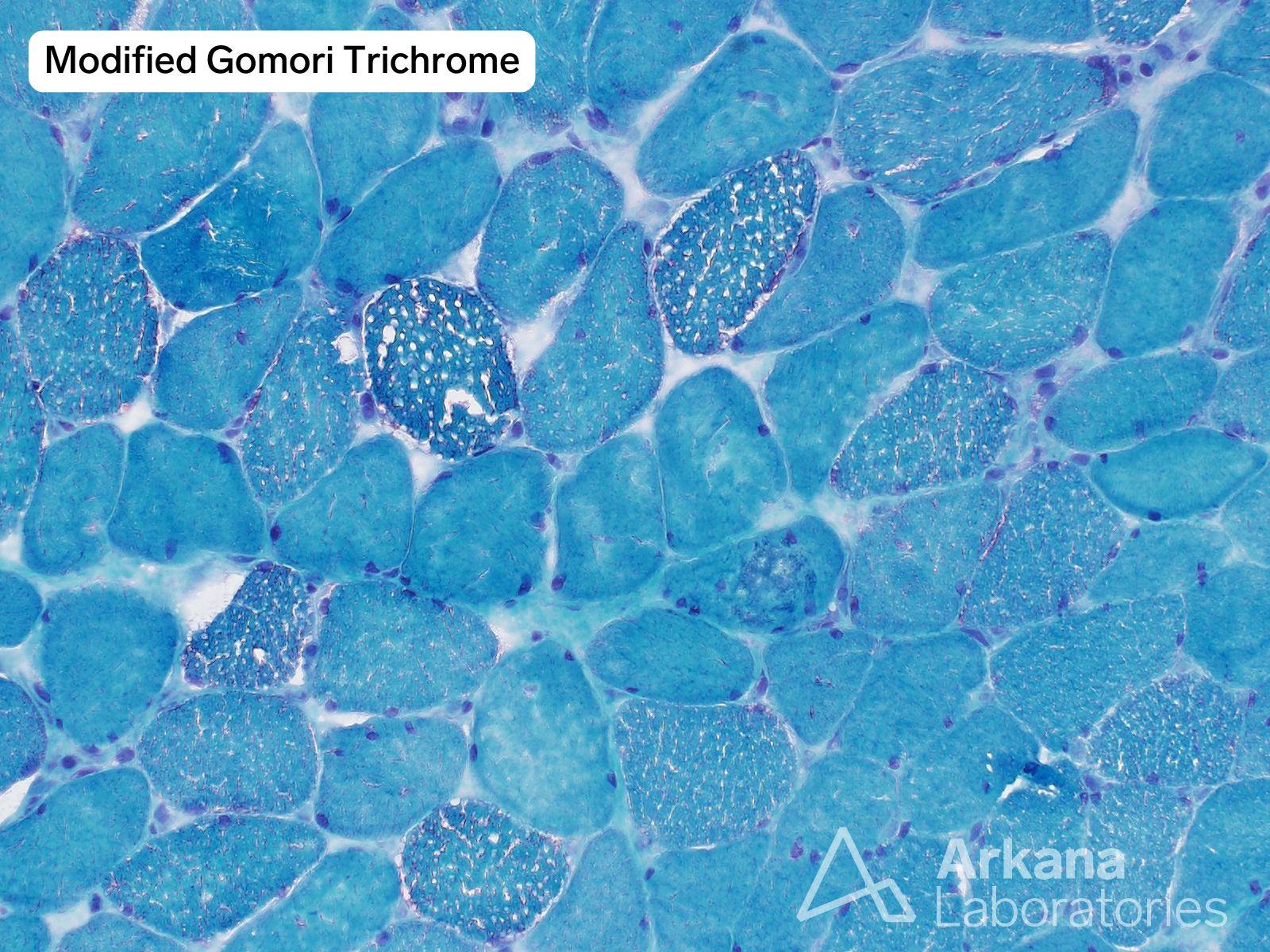
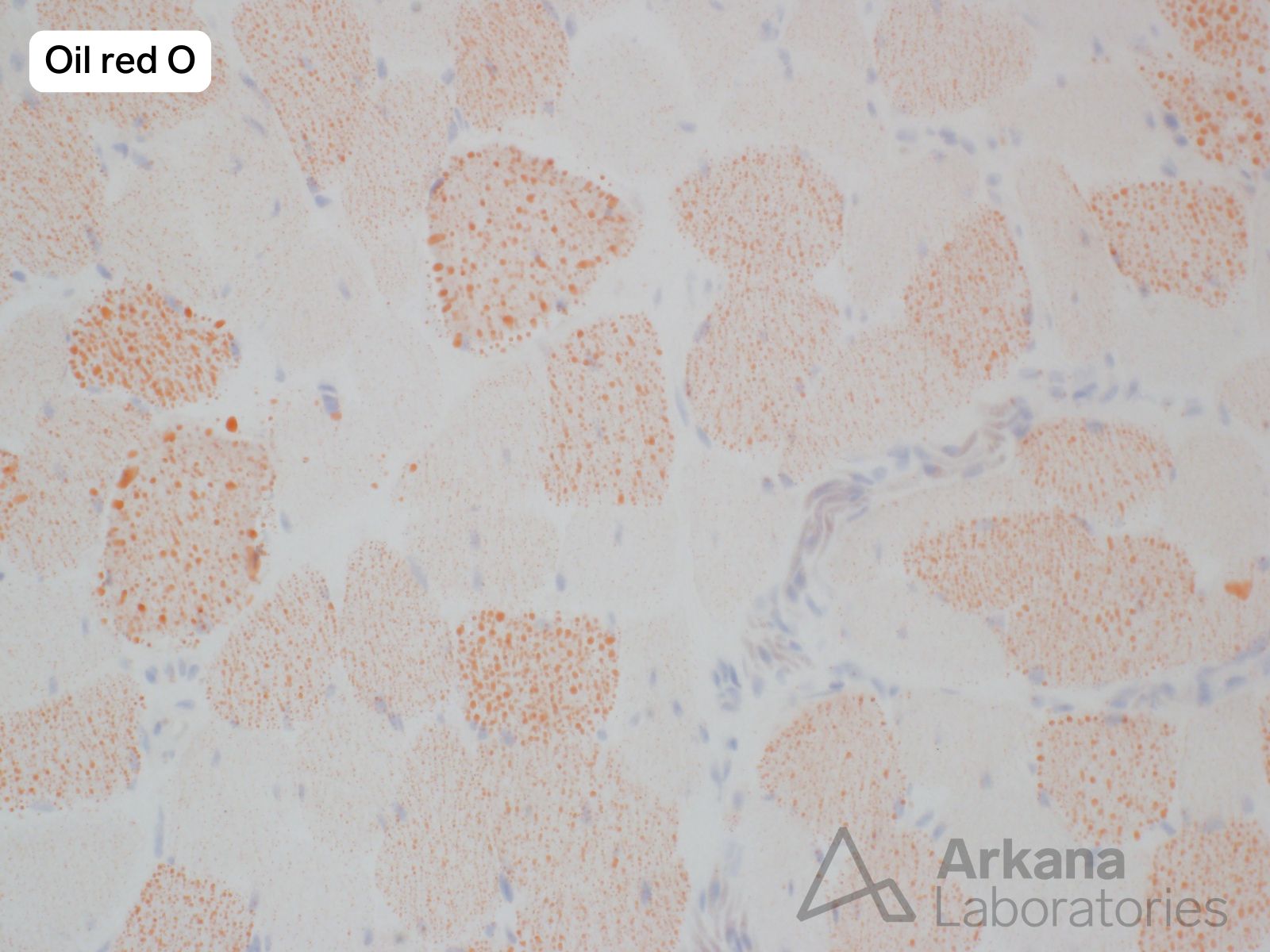
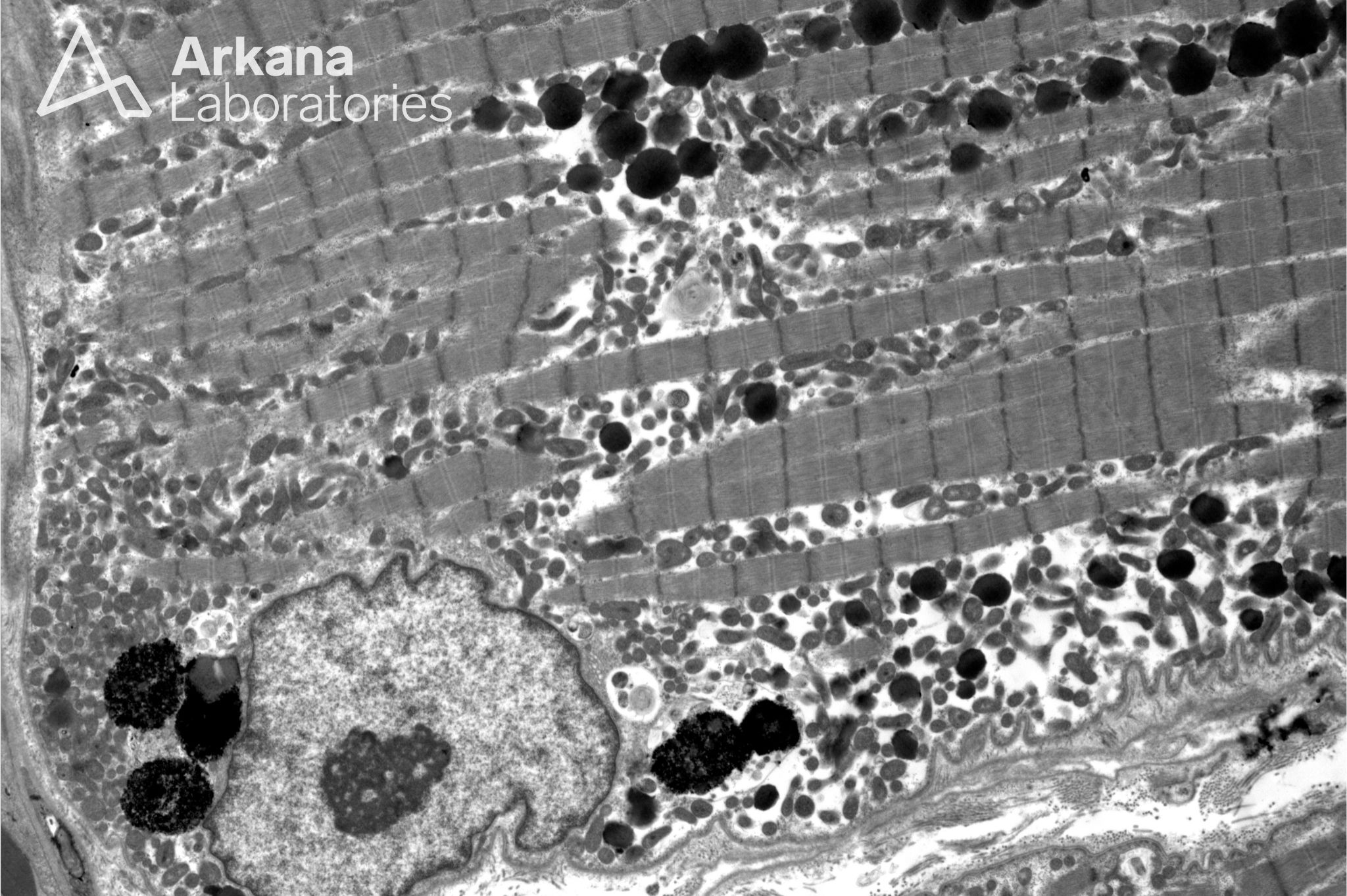
The overall pathologic changes are consistent with Lipid storage myopathy (LSM).
Subsequent laboratory testing results:
- Acylcarnitine profile: elevated levels of short-chain, medium-chain, and long-chain acylcarnitine species. Pyruvate kinase levels were within normal limits. This pattern could be associated with multiple acyl-CoA dehydrogenase deficiency (MADD) / glutamic acidemia type 2 (GA2) or carnitine-palmitoyltransferase II (CPT-II) deficiency / carnitine acylcarnitine translocated (CACT) deficiency. Defects of the mitochondrial respiratory chain or riboflavin deficiency should be considered as well.
- Pyruvate kinase: levels within normal limits.
These results support the morphologic impression of lipid storage myopathy.
The patient is reported to have shown some clinical improvement with riboflavin treatment.
Genetic testing is pending.
Lipid storage myopathy can occur in several settings, including genetic defects in components of the lipid metabolism pathway, mitochondria disorders and in the context of carnitine deficiency. Causes of LSM due to disorders in lipid metabolism pathway include Neutral Lipid Storage Disease of muscle (NLSD-M) due to mutations in the PNLA2 gene, riboflavin responsive Multiple Acyl-CoA Dehydrogenase Deficiency (RR-MADD) due to mutations in the ETFDH gene (Electron Transfer Flavoprotein Dehydrogenase), Carnitine Palmitoyltransferase 2 (CPT2) deficiency, and muscle carnitine deficiency (primary due to mutations in the SLC22A5 gene, or secondary). Late onset rr-MADD patients may manifest proximal myopathy, high CPK levels, vomiting and hypoglycemia, and typically respond well to riboflavin with carnitine supplementation.
Reference(s) / Additional Reading:
- Pennisi EM, Garibaldi M, Antonini G. Lipid Myopathies. J Clin Med. 2018 Nov 23;7(12):472. doi: 10.3390/jcm7120472. PMID: 30477112; PMCID: PMC6306737.
- Berardo A, DiMauro S, Hirano M. A diagnostic algorithm for metabolic myopathies. Curr Neurol Neurosci Rep. 2010 Mar;10(2):118-26. PMID: 20425236
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.