
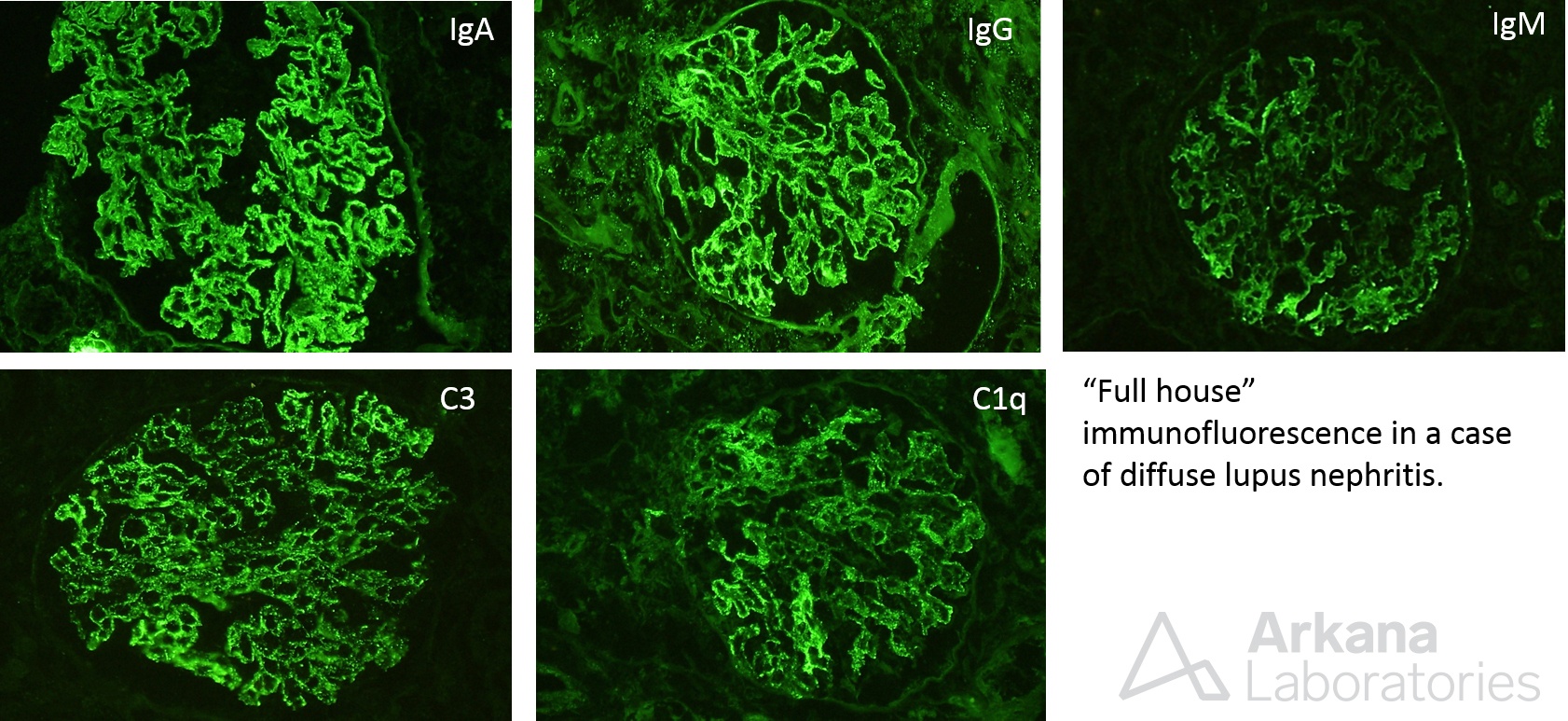
The above painting shows features of a proliferative glomerulonephritis. Endocapillary proliferation, crescent formation, and segmental sclerosis is shown. These findings can be seen in focal or diffuse lupus nephritis, but are not specific, as they can be identified in other proliferative glomerulonephritides, such as IgA nephropathy, infection-associated glomerulonephritis, and others. Immunofluorescence studies can help in distinguishing lupus from other forms of proliferative glomerulonephritis, as there is typically a “full house” pattern with expression of all 3 immunoglobulin heavy chains (IgA, IgM, IgG), and complement (C3, C1q), as shown below.
Classification of lupus nephritis is through the International Society of Nephrology / Renal Pathology Society (ISN/RPS) consensus criteria and includes 6 classes. These include minimal mesangial lupus nephritis (class I), mesangial proliferative lupus nephritis (class II), focal lupus nephritis (class III), diffuse lupus nephritis (class IV), membranous lupus nephritis (class V), and advanced sclerosing lupus nephritis (class VI).
This disease activity can be assessed on a renal biopsy using the modified NIH activity and chronicity indices (Bajema IM et al, 2018). Surrogates for disease activity include endocapillary hypercellularity, neutrophils or karyorrhexis within glomerular capillary loops, fibrinoid necrosis, hyaline deposits, cellular or fibrocellular crescents, and interstitial inflammation. Indicators of disease chronicity include the total percentage of global glomerulosclerosis, fibrous crescents, tubular atrophy, and interstitial fibrosis. These indices are helpful to compare activity and chronicity in repeat biopsies, as well as for standardized assessment for lupus clinical trials.
While treatment of a proliferative lupus requires immunosuppressive therapy, it remains unclear when to stop immunosuppression once a clinical remission is achieved. In a recent prospective cohort study, lupus patients with remission for over 1 year who have received 3 years of immunosuppressive therapy were re-biopsied and tapered off of therapy and followed for at least 2 years. All patients who had a flare following cessation of immunosuppression had a NIH disease activity index ≥2. The time since diagnosis of SLE as well as the NIH activity index may be helpful in predicting disease flares, as these were independent variables associated with increased flare risk in lupus patients (De Rosa M et al, 2018).
References:
Bajema IM, Wilhelmus S, Alpers CE, et al. Revision of the International Society of Nephrology / Renal Pathology Society classification for lupus: clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney International 2018; 93: 789-796.
https://www.ncbi.nlm.nih.gov/pubmed/29459092
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.
