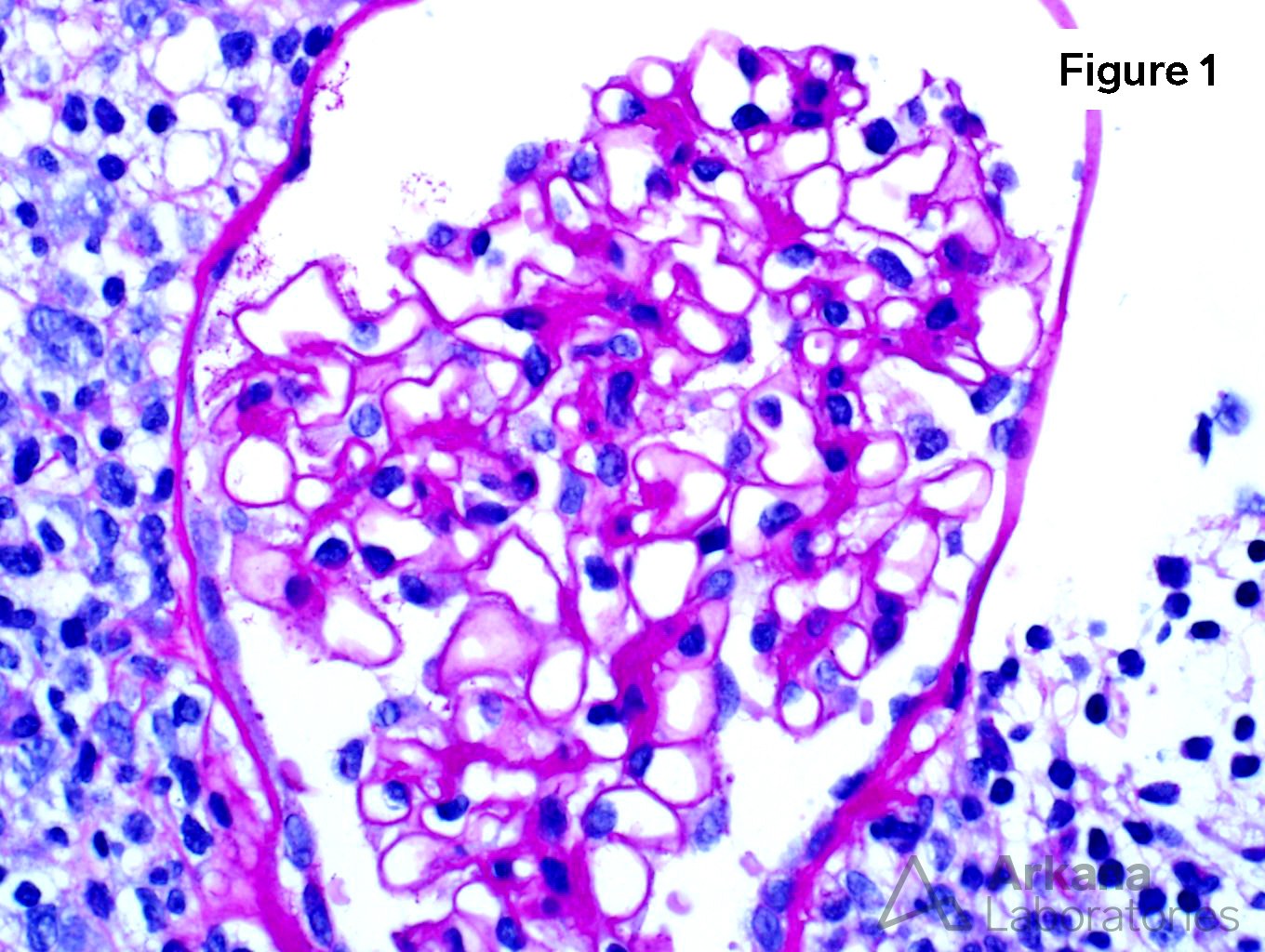
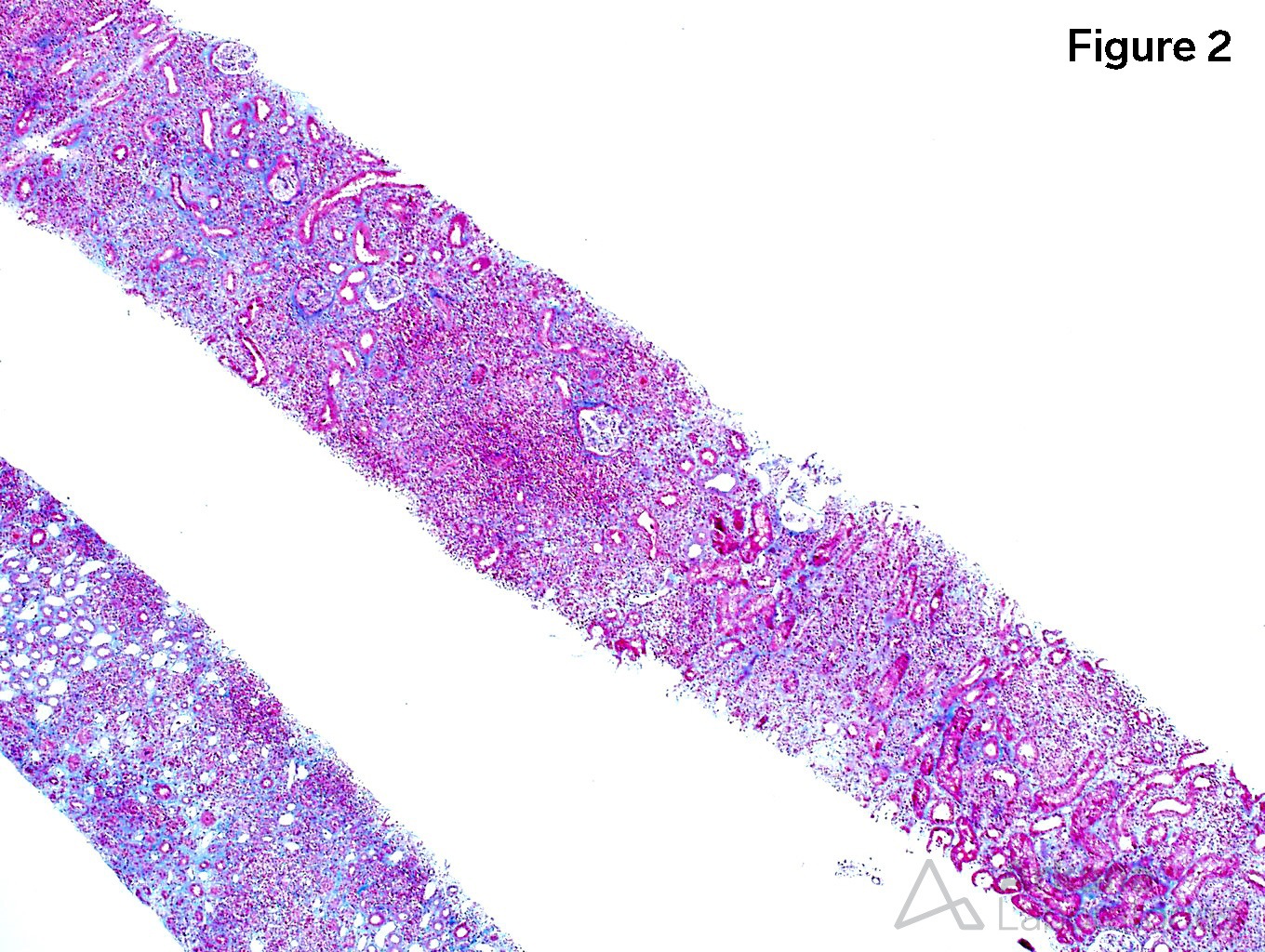
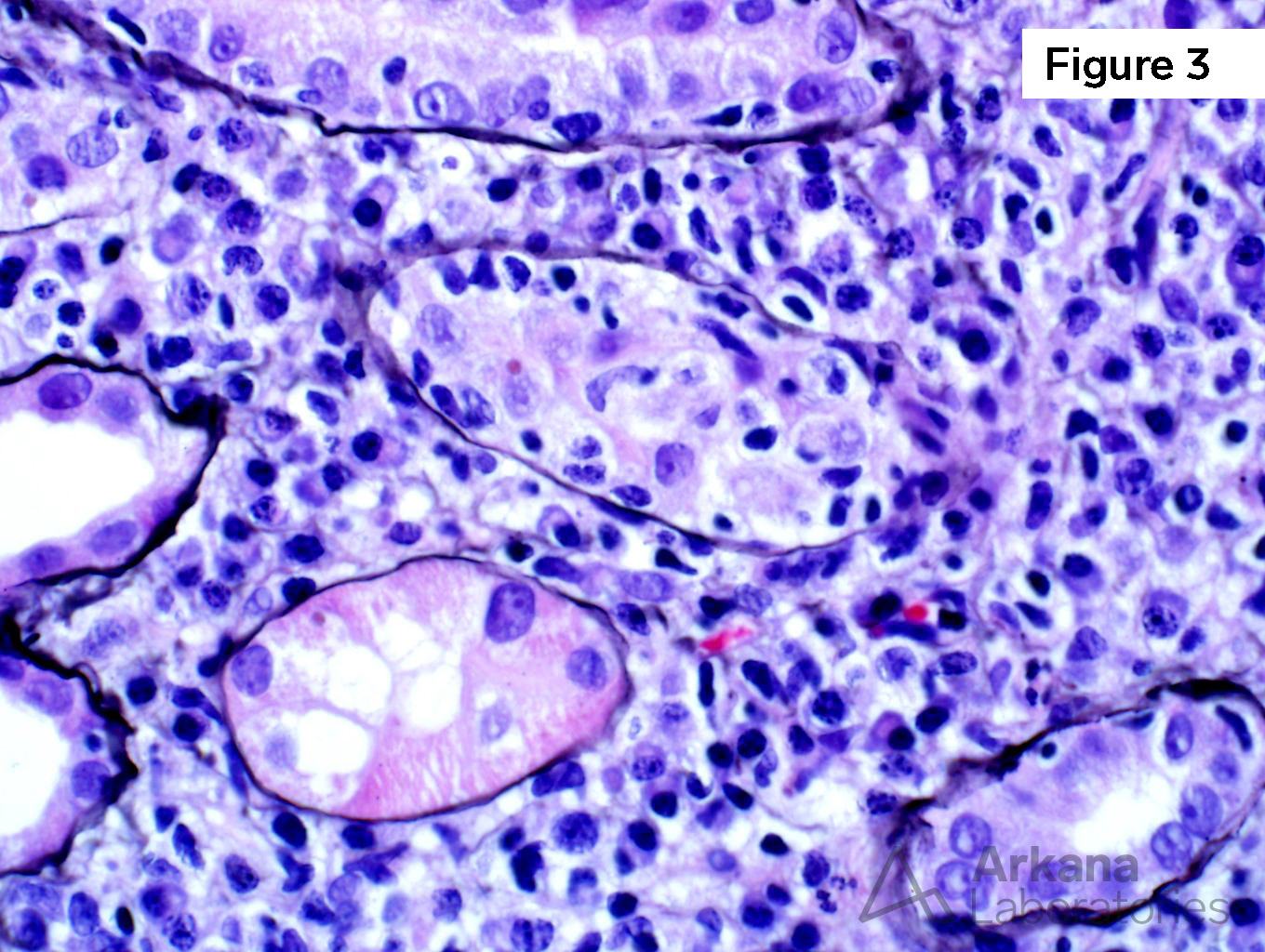
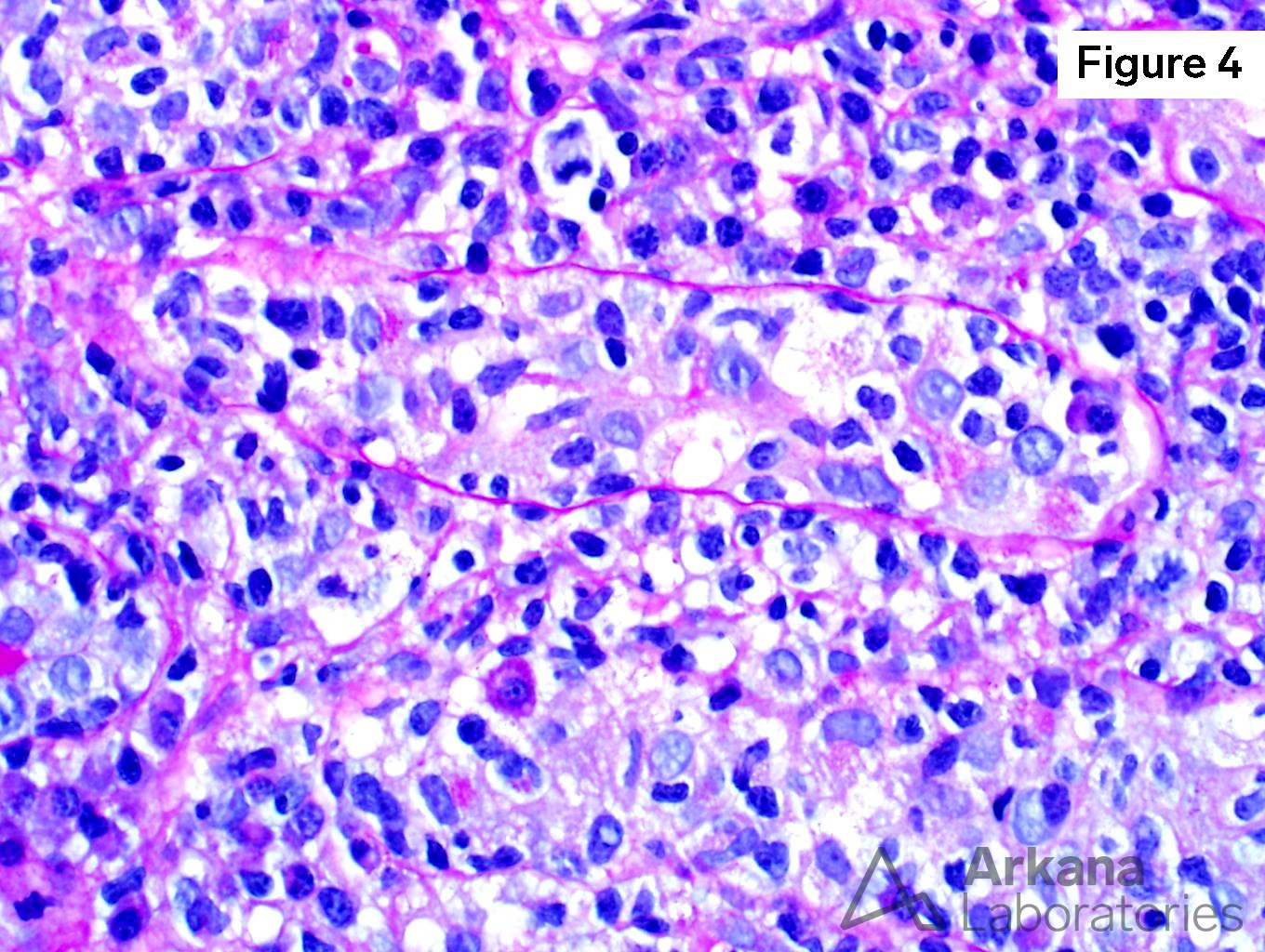
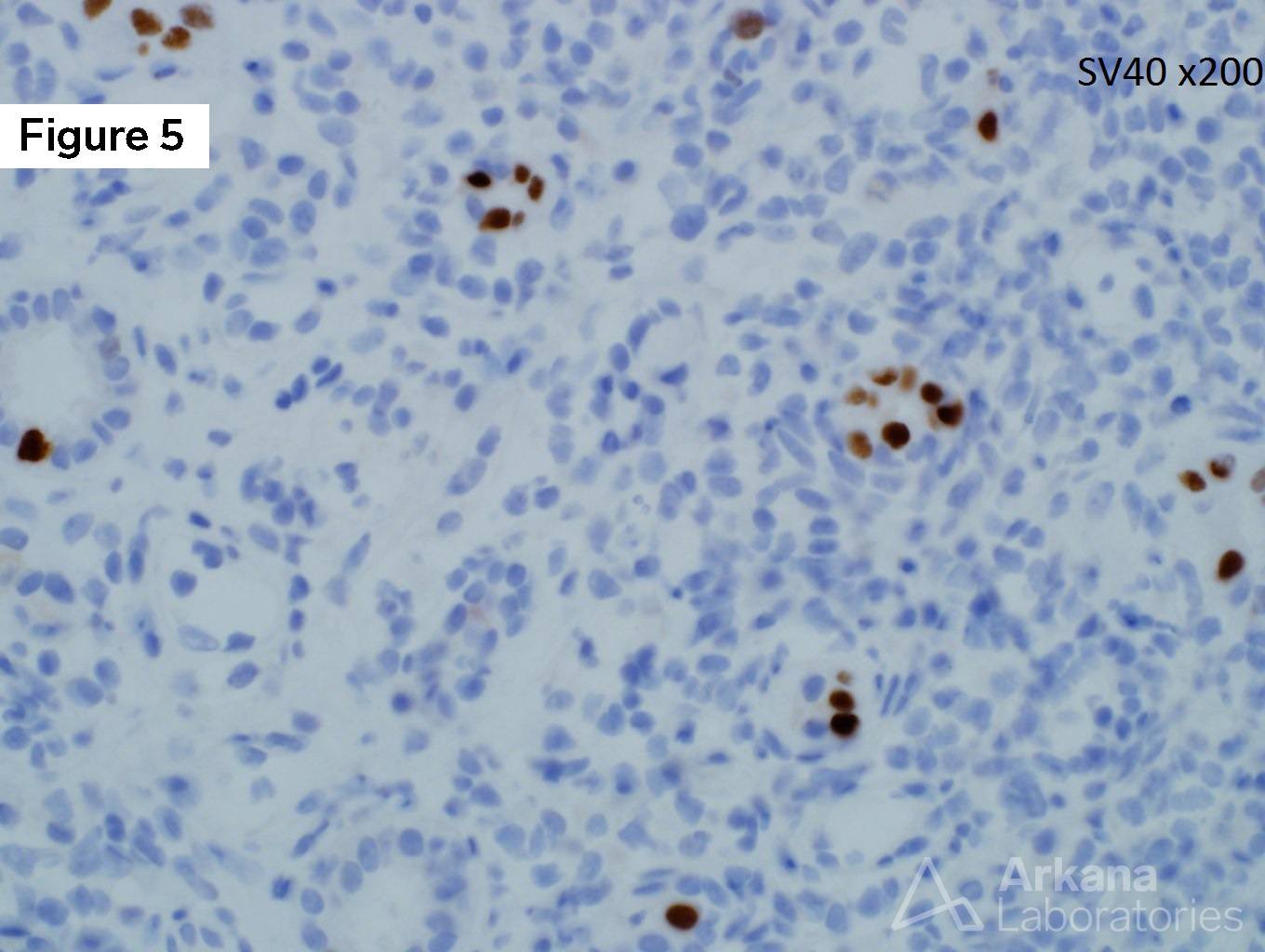
The patient is a 45-year-old male with a past medical history significant for ESKD secondary to IgA nephropathy S/P renal transplant (3 years ago). He has been in his normal state of health but presented with an abnormal creatinine of 2.5 mg/dL on routine examination. His BK viral load was elevated at 25,000 copies in the serum. Figure 1 shows a normal glomerulus, figure 2 shows severe interstitial inflammation, figures 3 & 4 show marked tubulitis, and figure 5 shows a SV40 positive stain.
This is a case of BK nephritis. BK virions are non-enveloped double-stranded DNA viruses. In immunohistochemistry, the antibody most commonly used is against the T antigen of SV-40 virus (simian polyomavirus), which cross-reacts both with BK virus and JC virus. In most transplant centers, the rate of BK nephritis is between 1-5% and plasma levels of >4 log10 c/mL are associated with an increased rate of biopsy proven BK nephritis. In kidney transplant recipients, approximately half of those with high-level viremia have biopsy-proven BK nephritis 2 to 6 weeks later. Since BK nephritis can be localized, it is estimated that there is a false-negative rate of 10-30% in biopsy samples. How exactly the virus spreads to the kidney and why certain patients with positive urine cytology become severely affected while others do not is unclear. Polyomavirus nephropathy is usually a progressive disease and treatment depends on reducing the amount of immunosuppression.
https://www.ncbi.nlm.nih.gov/pubmed/30859620
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.