Clinical Presentation
A 65-year-old male with a medical history of hypertension and hyperlipidemia presented with lower extremity edema ongoing for two months. Laboratory investigations revealed a serum creatinine level of 5 mg/dL and proteinuria of 4 g/day. Microscopic examination of the urine sediment showed numerous granular casts. Given the clinical presentation and laboratory findings, a renal biopsy was performed.
Renal Biopsy Findings:
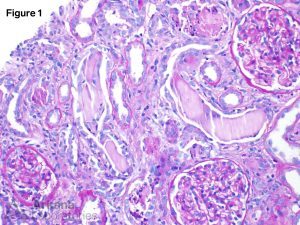
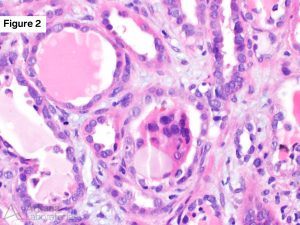

The renal biopsy specimen revealed extensive tubular injury characterized by the presence of intratubular casts. These casts appeared pale when stained with periodic acid-Schiff (PAS) and occasionally displayed a fractured pattern along with cellular reaction (Figure 1 and 2). Additionally, a background of moderate interstitial fibrosis and tubular atrophy, accompanied by an inflammatory reaction, was observed. Immunofluorescence staining demonstrated positive reactivity for kappa light chains within the tubular casts. In contrast, no staining for lambda light chains was detected in the casts (Figure 3). Notably, all immunofluorescence stains in the glomeruli were negative. Congo red staining, used to detect the presence of amyloid deposits, was also negative.
Diagnosis: Light chain cast nephropathy
The morphologically atypical casts showing kappa light chain restriction on immunofluorescence confirmed the diagnosis of light chain cast nephropathy (LCCN). LCCN represents a type of renal injury caused by the deposition of monoclonal immunoglobulin light chains within the renal tubules, resulting in renal dysfunction. The pathogenesis involves the production of monoclonal immunoglobulin light chains by clonal plasma cells, which subsequently filter through the glomeruli and deposit within the renal tubules. Tubular injury occurs due to both the toxic effects of the light chains on tubular cells and the obstruction of tubular lumens by the casts. LCCN is frequently referred to as myeloma cast nephropathy due to its strong association with multiple myeloma. In fact, LCCN was the initial renal lesion described in patients with myeloma and remains the leading cause of acute renal failure in individuals diagnosed with myeloma.
The presence of atypical intratubular casts, characterized by their crystalline appearance, weak or negative PAS staining, and cellular reaction, should raise suspicion for LCCN. Testing for light chain restriction through immunofluorescence should be performed. It is important to note that certain drugs, such as vancomycin, rifampin, tacrolimus, and rapamycin, can induce tubular injury with casts that resemble those seen in LCCN. However, these drug-related casts will test negative for monoclonal light chains. Moreover, casts composed of myoglobin and hemoglobin, observed in the context of rhabdomyolysis and intravascular hemolysis, respectively, can mimic light chain casts. Immunohistochemical staining for myoglobin and hemoglobin aids in differentiating these entities from LCCN.
References:
Dvanajscak Z, Cossey LN, Larsen CP. A practical approach to the pathology of renal intratubular casts. Seminars in Diagnostic Pathology. 2020;37(3):127-134.
Jennette JC, Olson JL, Silva FG, D’Agati V, Heptinstall RH *1920 *, eds. Heptinstall’s Pathology of the Kidney: Includes Interactive EBook with Complete Content. Seventh edition. Wolters Kluwer; 2015.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.