Ganglioglioma (GG)
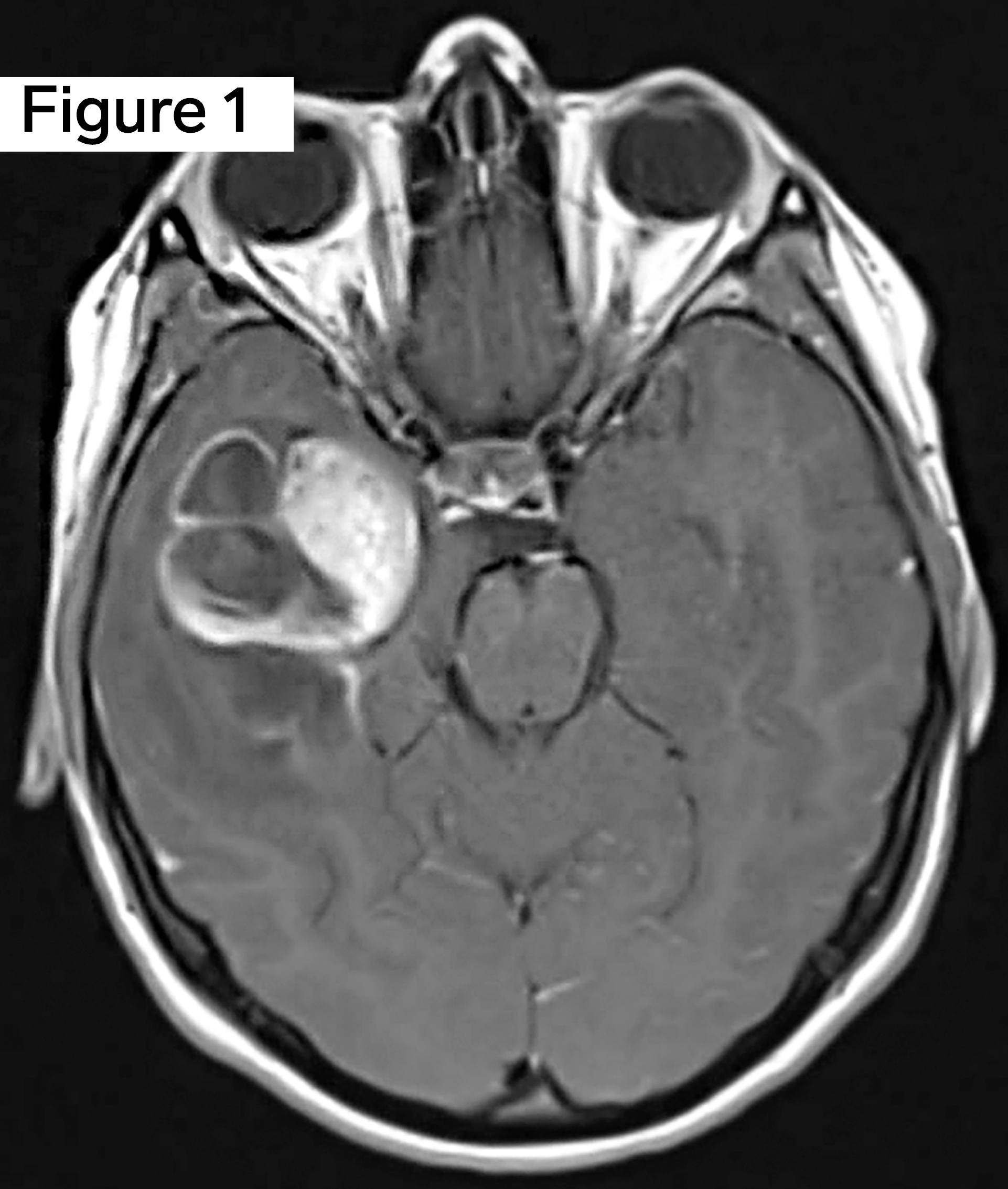
A young adult female presents with generalized headaches of several months duration, which recently progressed in intensity with associated nausea and vomiting. She was in previously good health without significant past medical history. Neuroimaging with MRI Brain demonstrated a 4 cm multicystic mass with calcifications in the right temporal lobe. Neurosurgery pursued craniotomy and resection. Using the figures above, what is your diagnosis of this low-grade cystic brain tumor?
Answer: Ganglioglioma (GG)
This brain tumor is a classic example of a Ganglioglioma (GG), WHO grade I, answer choice (C).
Per 2016 WHO Classification of CNS Tumors, revised 4th ed., gangliogliomas (GGs) are classified as mixed neuronal-glial tumors defined as well-differentiated slow-growing neoplasms composed of dysplastic ganglion cells in combination with neoplastic glial cells.
Gangliogliomas (GGs) tend to present in the temporal lobes of children and young adults and are commonly associated with early-onset focal epilepsy/seizures.
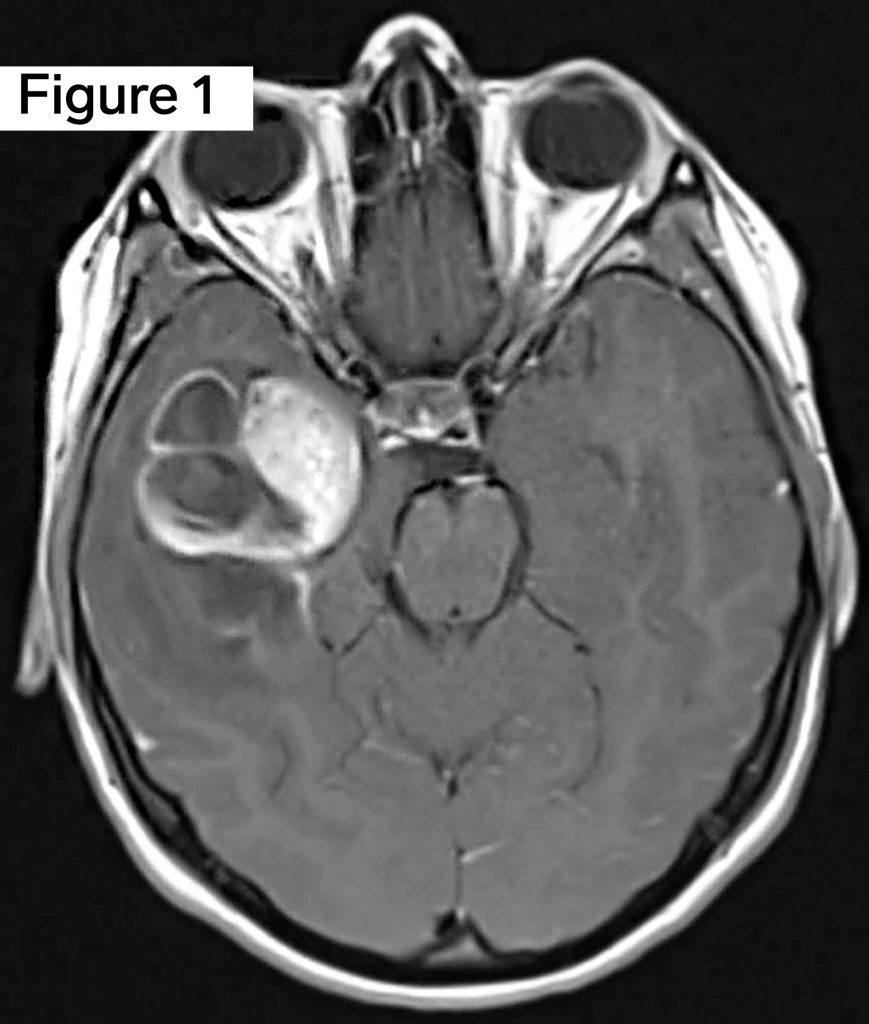
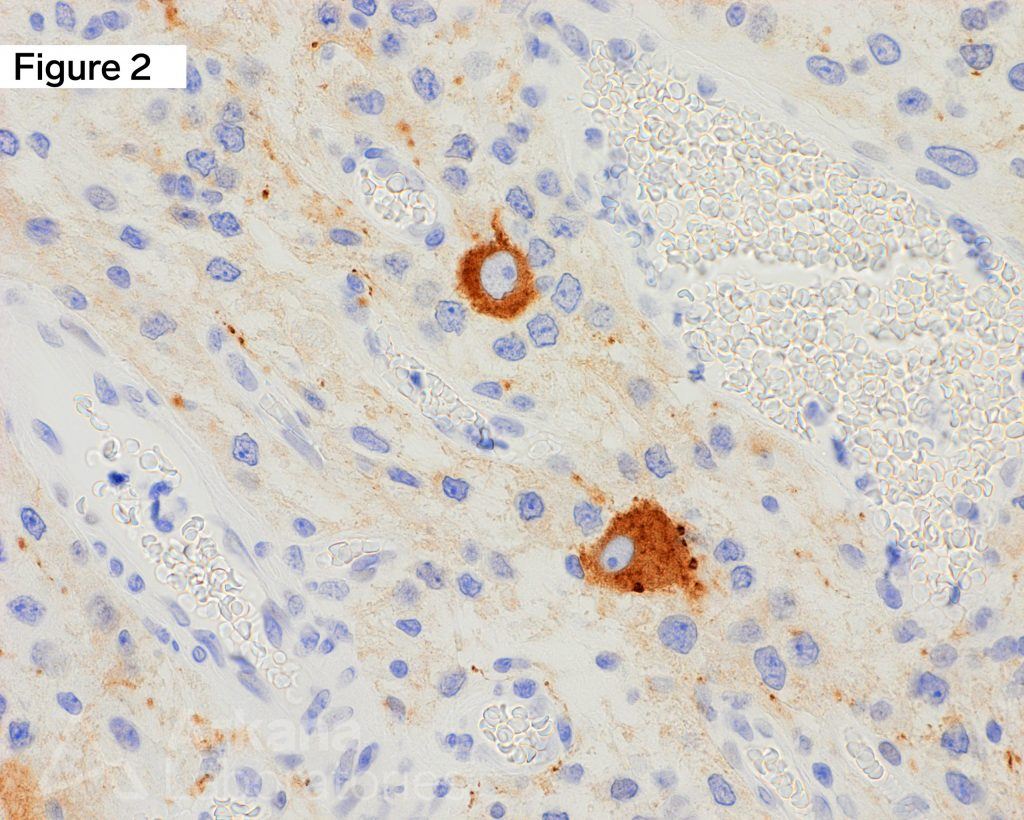
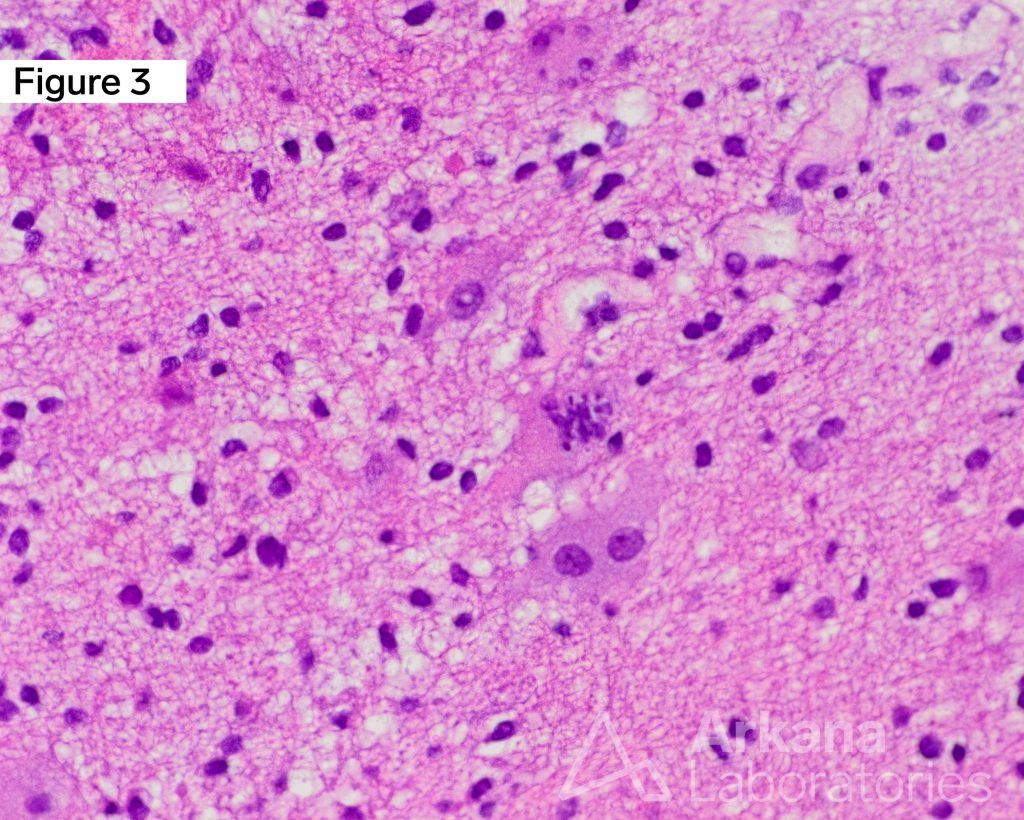
Young adult female with headache and a cystic brain tumor in the right temporal lobe. Figure 1 is an MRI Brain image in the T1 sequence post-contrast in the axial plane, which demonstrates a ~4 cm multicystic mass in the medial right temporal lobe with a solid mural nodular component with heterogeneous enhancement of the solid portions and cystic rim. Calcifications are noted along with the septal and wall components (not well demonstrated in the image shown). Figure 3 is a hematoxylin and eosin (H&E)-stained section of formalin-fixed paraffin-embedded (FFPE) tissue demonstrating a low-grade glioneuronal tumor containing dysplastic ganglion cells with a background glioma component composed of numerous delicate piloid astrocytes, reminiscent of pilocytic astrocytoma. An exceedingly rare coarse mitotic figure is seen. Figure 2 is an immunohistochemical (IHC) stain for Synaptophysin, which shows strong immunoreactivity in the dysplastic ganglion cell component of the tumor. Original magnifications: A. MRI T1 Ax Post-Con; B. H&E, 400x; C. IHC stain for Synaptophysin, 400x.
Why were the other answers wrong?
The other answer choices (pleomorphic xanthoastrocytoma [PXA], pilocytic astrocytoma [PA], and dysembryoplastic neuroepithelial tumor [DNET]) absolutely enter the differential diagnosis of cystic brain tumors of the temporal lobes in children and young adults, especially when associated with epilepsy/seizures.
Each of these tumors is defined by its own unique histopathologic findings, as well as incorporation of an integrated diagnosis that may include molecular and/or cytogenetic alterations.
However, this case shows classic histopathologic findings unequivocally diagnostic of a ganglioglioma (GG).
References
Becker AJ, et al. Ganglioglioma. In: WHO classification of tumors in the central nervous system, 2016 revised 4th ed. Edited by DN Louis, et al. IARC Press, Lyon, France. 2016: 138-141.
Pekmezci M, Villanueva-Meyer JE, Goode B, et al. The genetic landscape of ganglioglioma. Acta Neuropathol Commun. 2018 Jun 7;6(1):47. PMID: 29880043.
Provenzale JM, Ali U, Barboriak DP, et al. Comparison of patient age with MR imaging features of gangliogliomas. AJR Am J Roentgenol. 2000 Mar;174(3):859-62. PMID: 10701639.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.