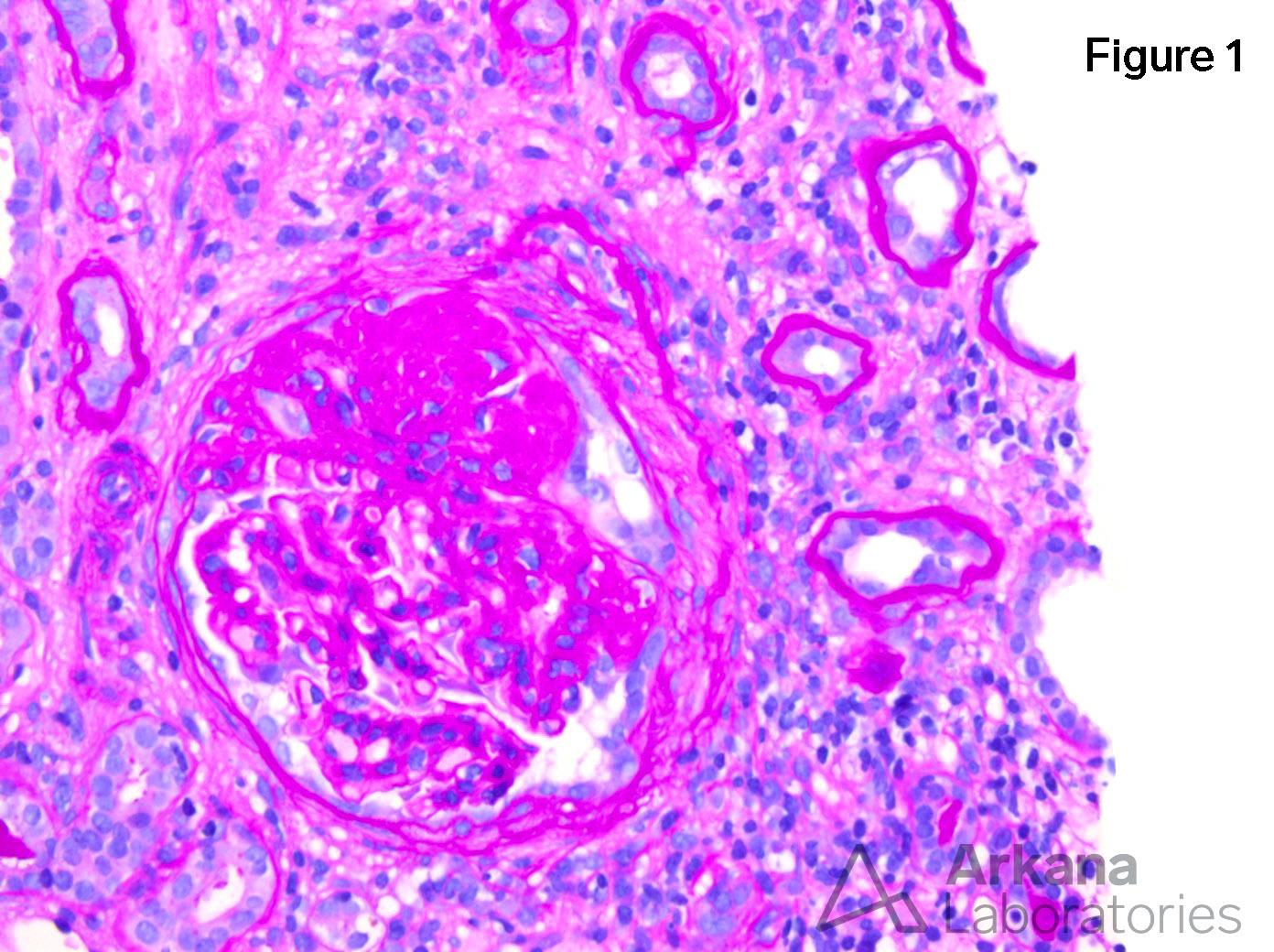
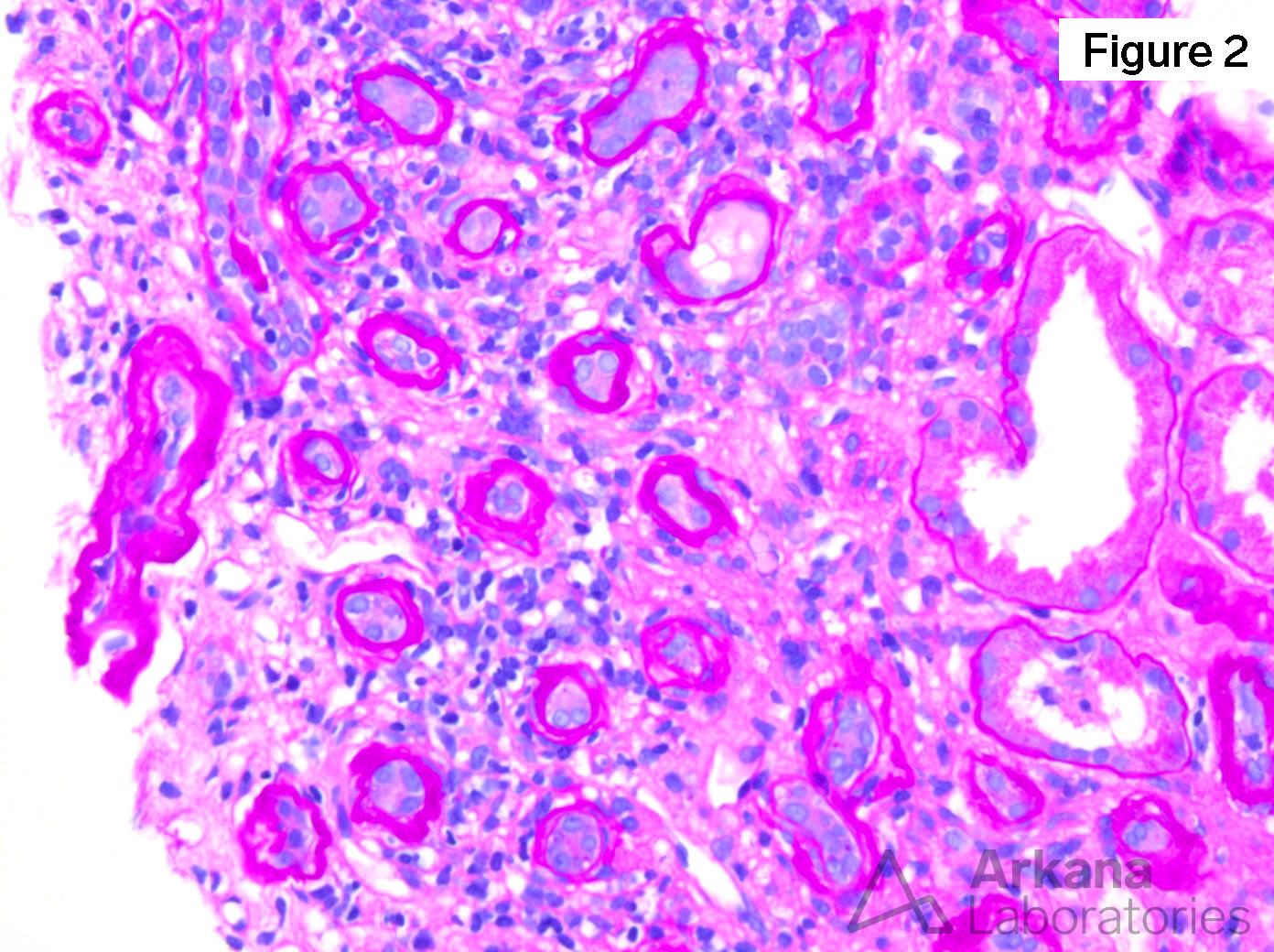
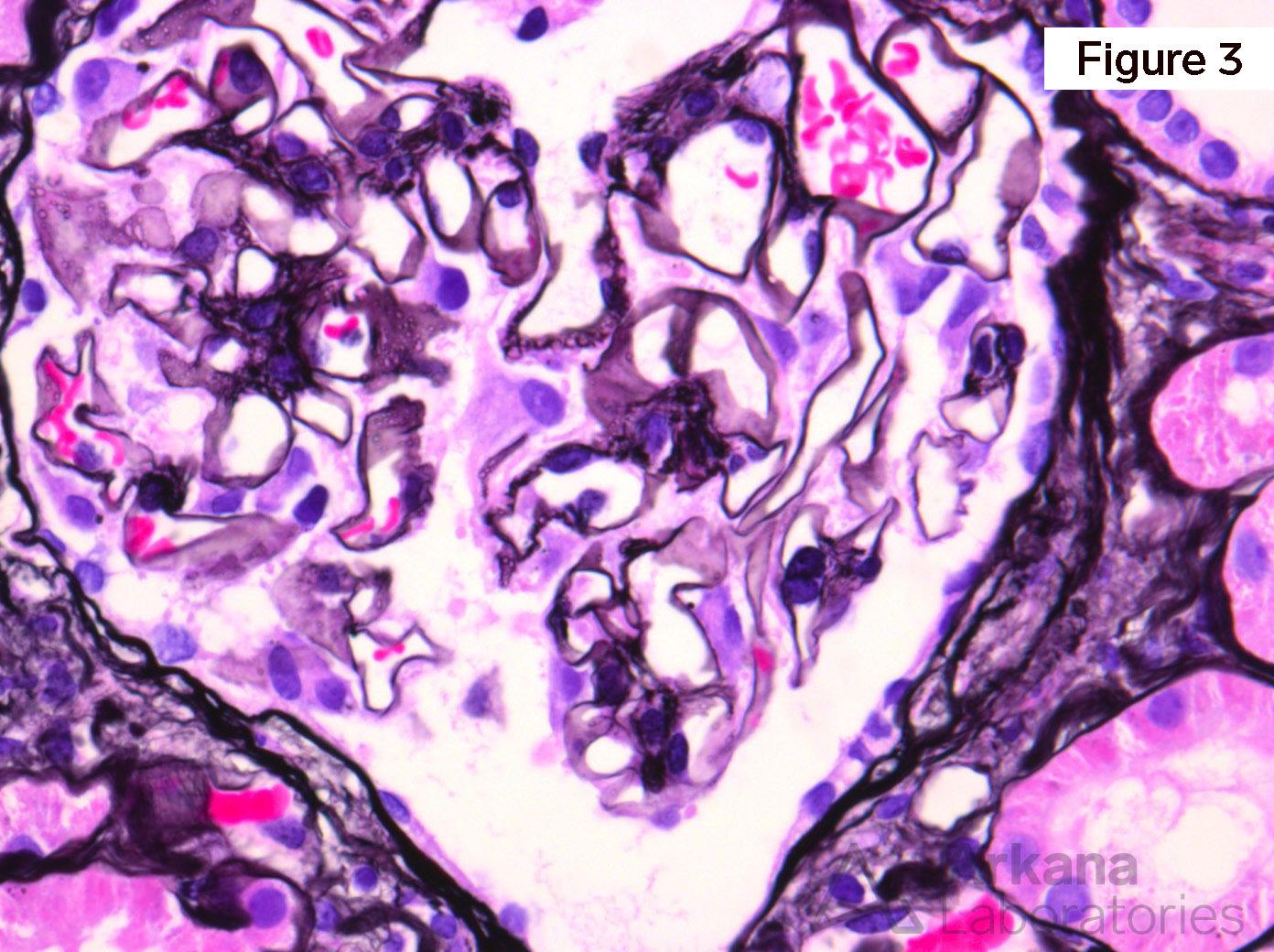
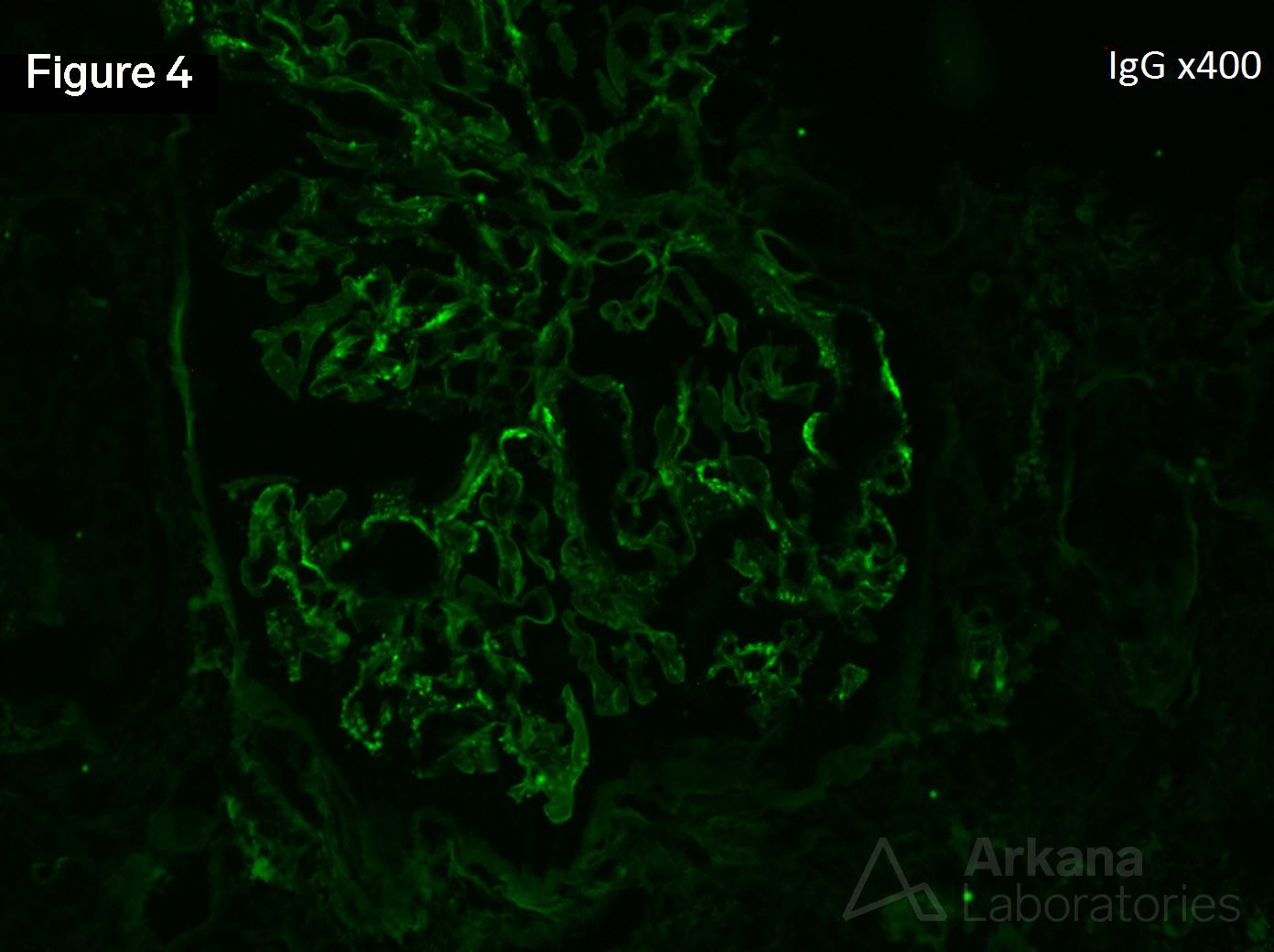
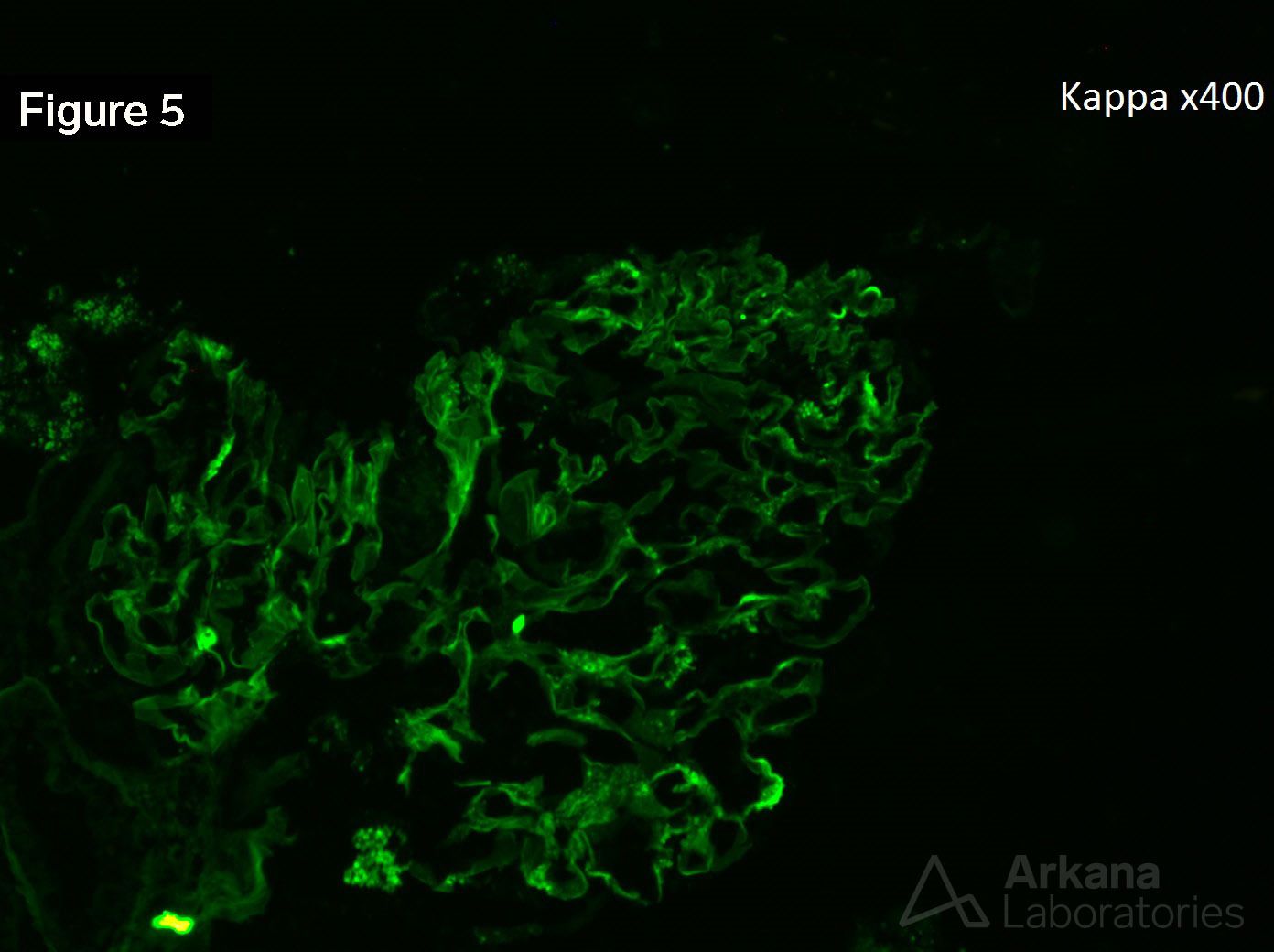
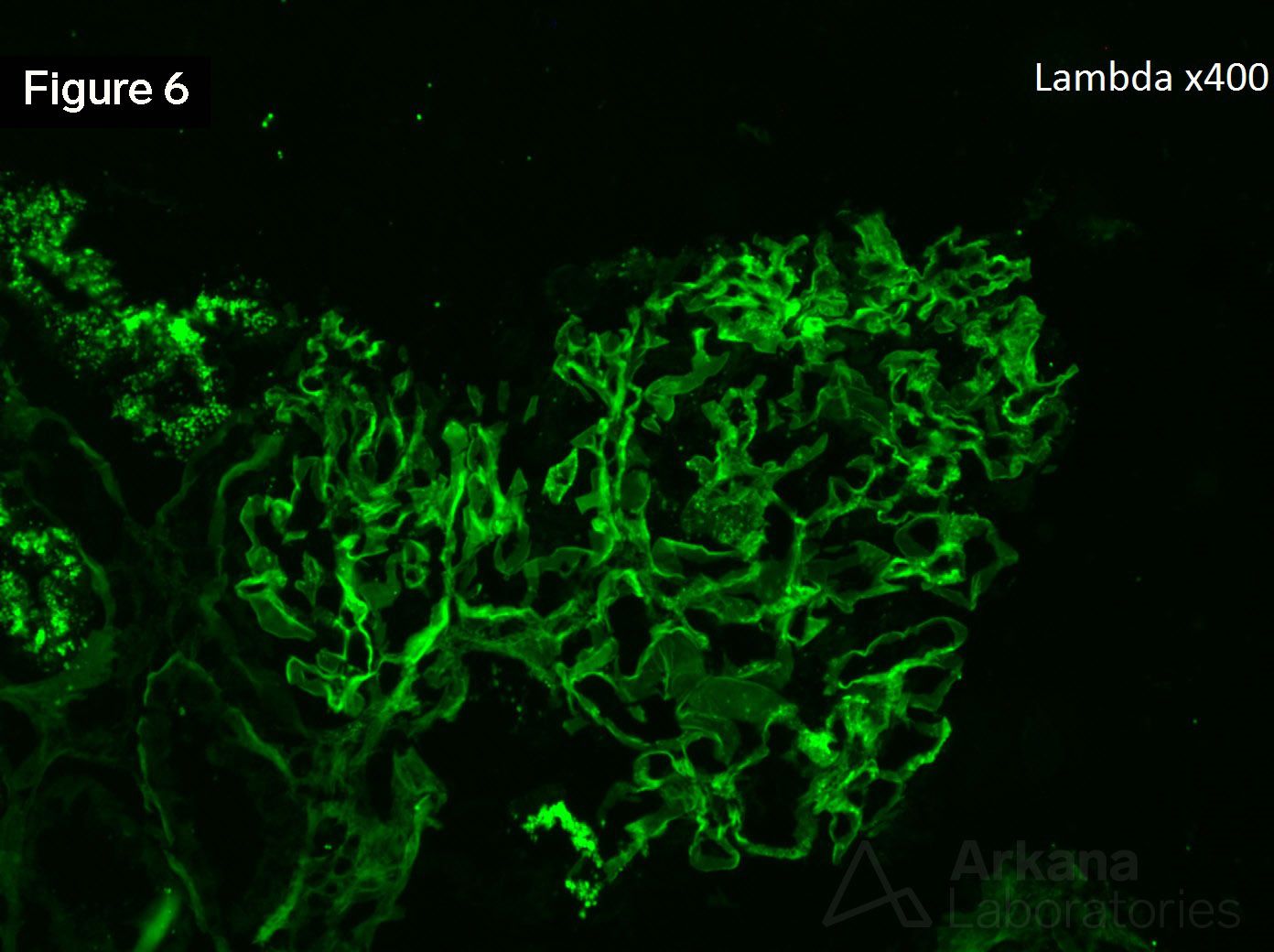
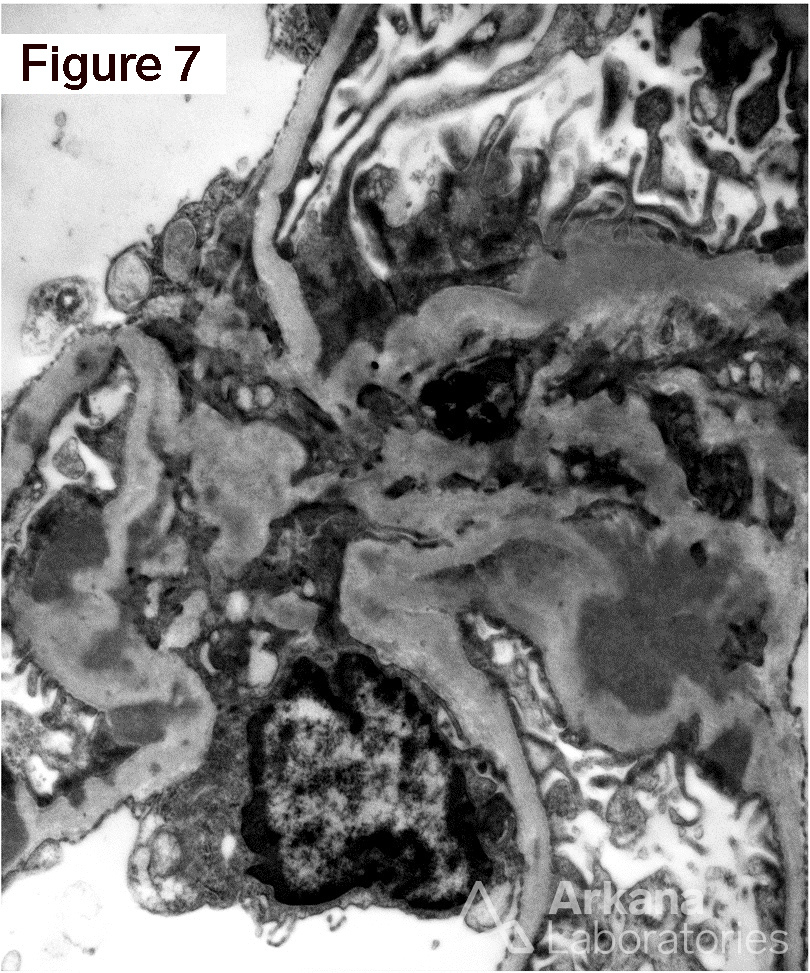
The patient is a 24 year-old African American male who has recently been diagnosed with HIV infection. He has not received HAART therapy and presents to the hospital with 1.2 g/g of proteinuria and a creatinine of 2.9 mg/dL. Figure 1 shows segmental sclerosis. Figure 2 shows tubular atrophy and interstitial inflammation. Figure 3 shows “hole” formation in glomerular basement membranes. Figures 4, 5, and 6 shows IgG, kappa, and lambda, respectively. Figure 7 shows mesangial and capillary wall electron dense deposits. This is a case of HIV immune complex disease of the kidney (HIVICK).
HIV immune complex disease of the kidney is a constellation of histopathological diseases found in patients who are HIV positive. Approximately 50% of glomerular histology in HIVICK can be described as infection-associated glomerulonephritis while the remaining half consists of membranous, IgA, MPGN, and “lupus-like” diffuse proliferative glomerulonephritis. IgA has been included in this group because studies have shown colocalization of the HIVp24 and gp120 antigens with IgA in the presence of active HIV infection. In general, HIVICK progresses at a much slower rate than HIV-associated nephropathy with 32% of patient’s progressing to ESRD in 2 years. “Lupus-like” proliferative lesions and membranous lesions progress the fastest in this group of lesions. The majority of studies have not shown a major effect of HAART therapy on treatment of HIVICK.
https://www.ncbi.nlm.nih.gov/pubmed/27797895
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.