Clinical History:
- 49-year-old man presents to the Emergency Department with aphasia
- MRI reveals a 4 cm T2/FLAIR bright, gadolinium enhancing mass lesion in the posterior left frontal lobe with involvement of the corpus callosum
- Neurology and Interventional Neuroradiology clear patient as unlikely to represent ischemic lesion
- Neurosurgery is consulted and elects for biopsy the next morning
Question:
Definitive diagnosis will require additional viable tissue for what testing?
A. 1p / 19q chromosome co-deletion
B. IDH mutation status
C. CDKN2A/B homozygous deletion
D. EGFR amplification

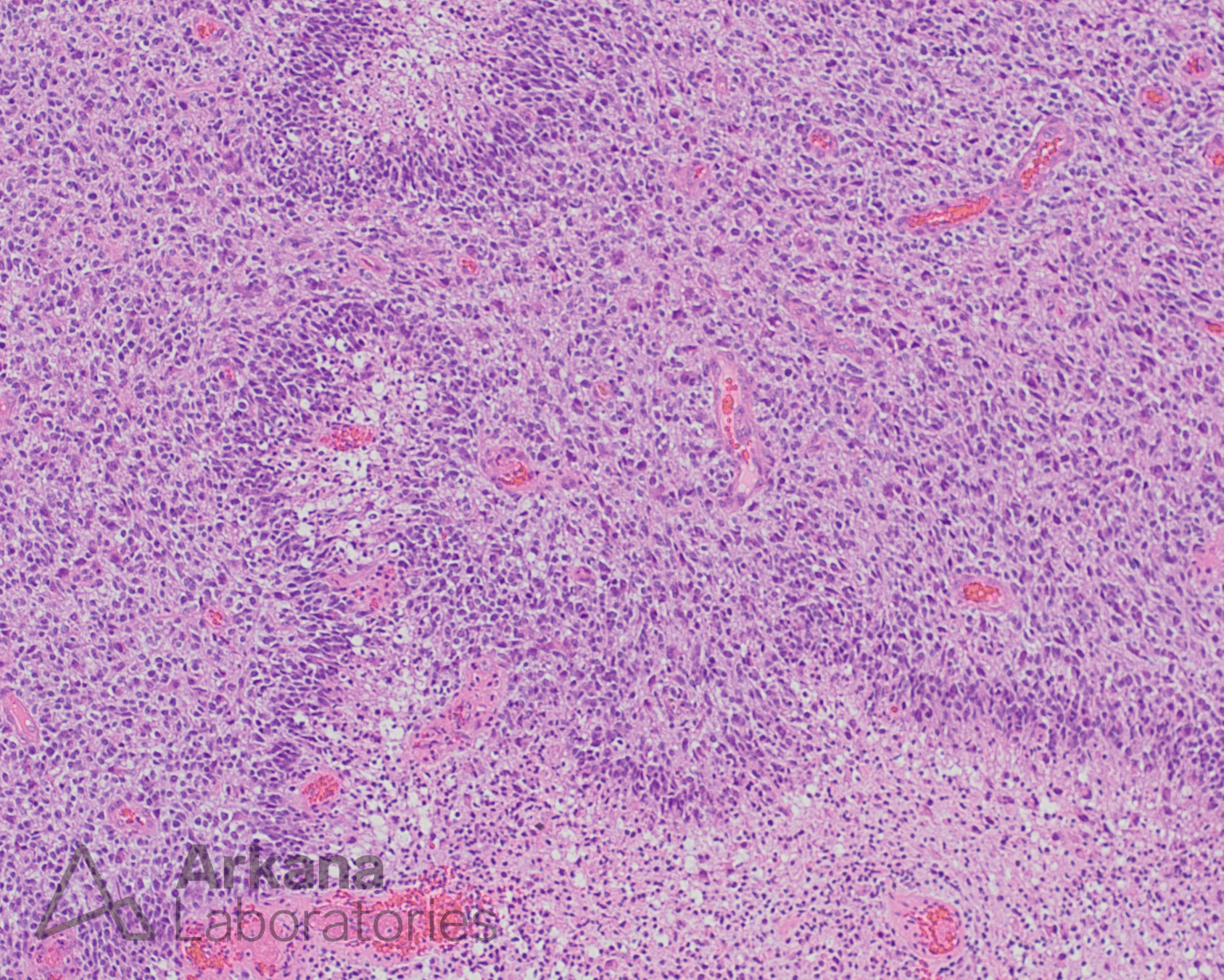
Figure 1: Neuropathology receives the following tissue for intraoperative consultation
Answer:
Definitive diagnosis will require additional viable tissue for what testing?
B. IDH mutation status <– correct answer
GBM Necrosis
Eosinophilic granular necrosis with thrombotic vessels (arrow) is essentially pathognomonic for glioblastoma in the setting of brain biopsies. Additional viable tissue will be required for definitive diagnosis. A reasonable intraoperative diagnosis: “Necrosis, suspicious for high-grade glioma; additional tissue requested.”
Glioblastoma histology
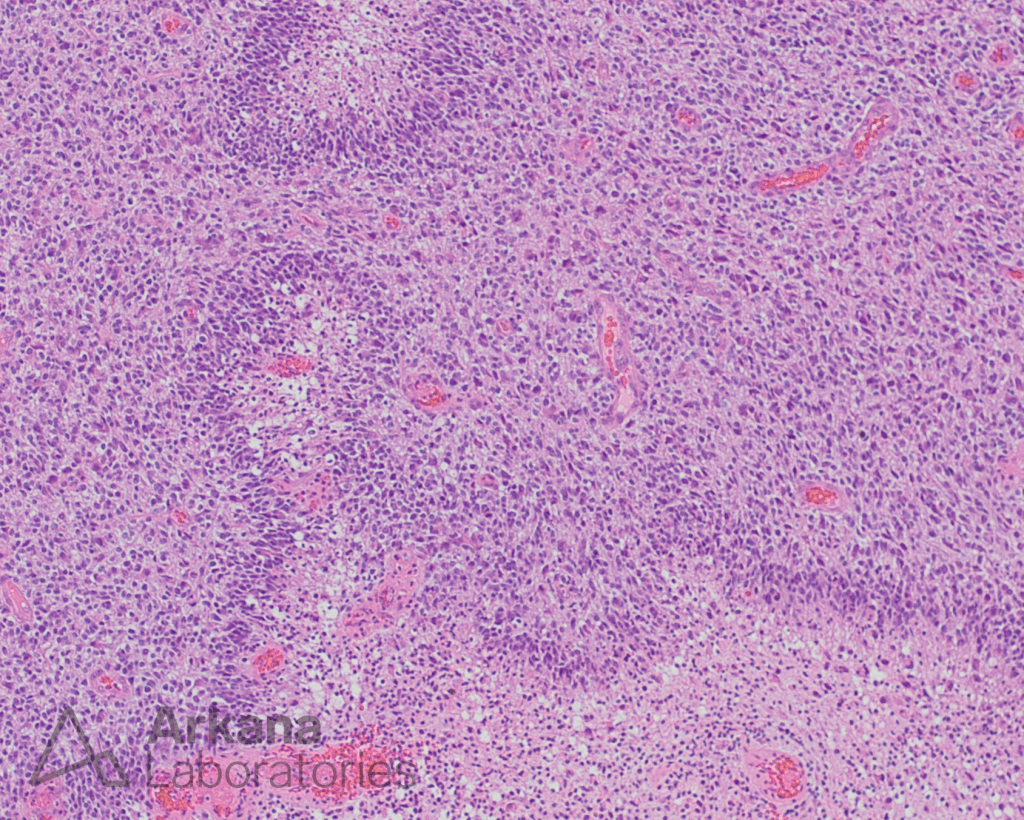
Infiltrating astrocytic neoplasm characterized by palisading necrosis and/or vascular proliferation
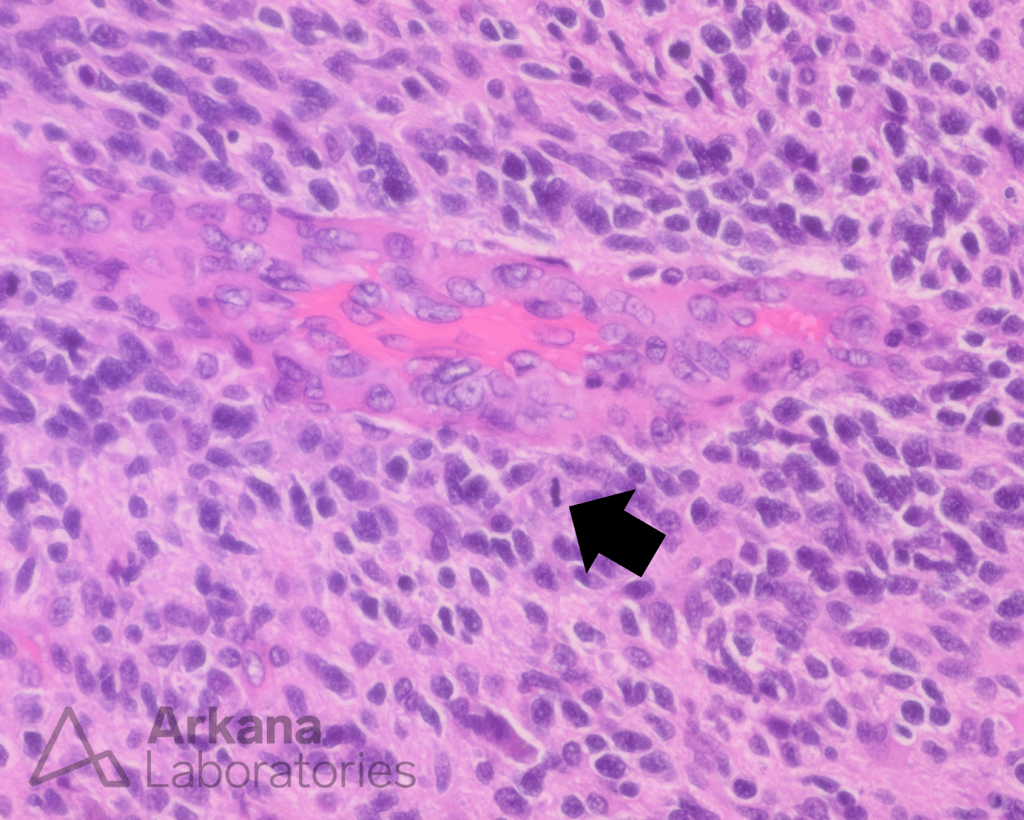
Mitotic figures (black arrow) are also expected to be present.
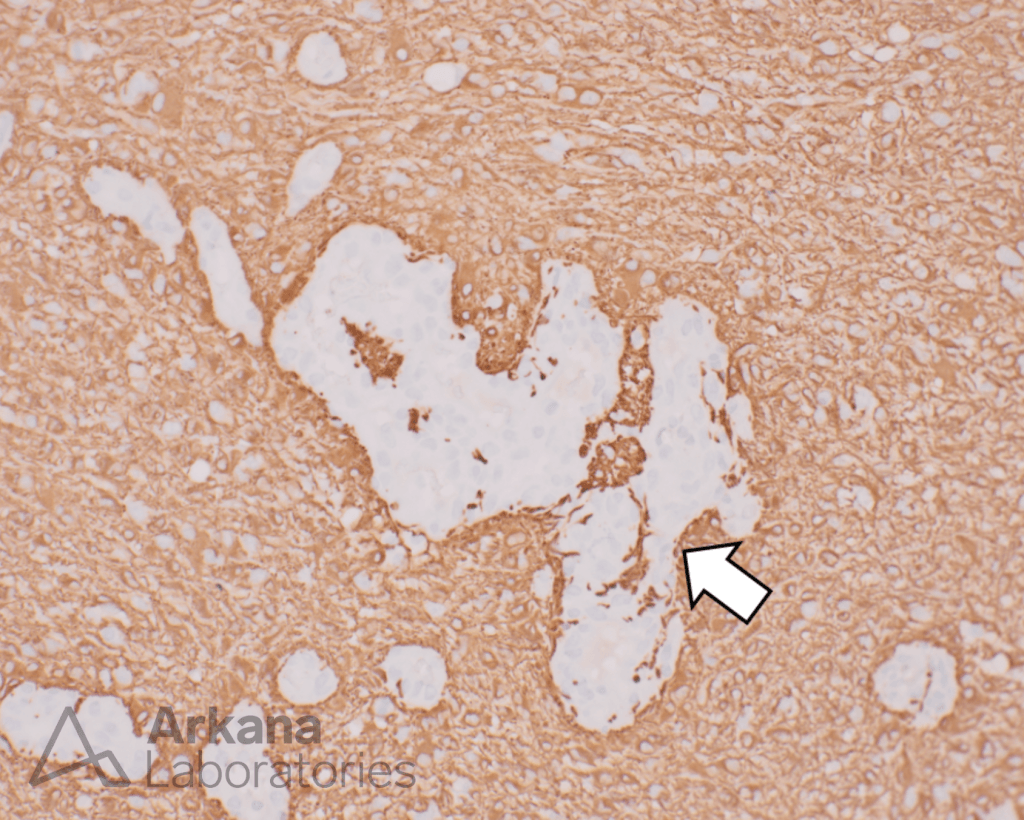
GFAP immunoreactivity is also expected in the vast majority of tumors and can negatively highlight vascular proliferation (white arrow).
Testing in Glioblastoma
Multiple additional tests are desirable for the full characterization of a new diagnosis of glioma; however, IDH mutation status is required for the definitive diagnosis of infiltrating whenever possible.
IDH mutation status has dramatically different prognostic implications for patients with IDH wild-type tumors behaving more aggressively.
IDH-mutant tumors should be tested for CDKN2A/B homozygous deletion as these tumors have a significantly less favorable prognosis.
Reference(s) / additional reading:
WHO Classification of Tumours Editorial Board. World Health Organization Classification of Tumours of the Central Nervous System. 5th ed. Lyon: International Agency for Research on Cancer; 2021.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.