This middle-aged patient presented with complaints of proximal muscle weakness, myalgias, and skin rash (face and chest) of several months duration. Laboratory studies demonstrated elevated CPK (585), aldolase (8.6), and CRP. Myositis-specific autoantibody panel was positive for NXP2 and TIF1-gamma autoantibodies. The patient was treated with methotrexate and prednisone prior to muscle biopsy.
Based on the clinical history and Figures #1 and #2, what is your diagnosis?
A. Normal muscle
B. Polymyositis
C. Necrotizing myopathy
D. Treated dermatomyositis
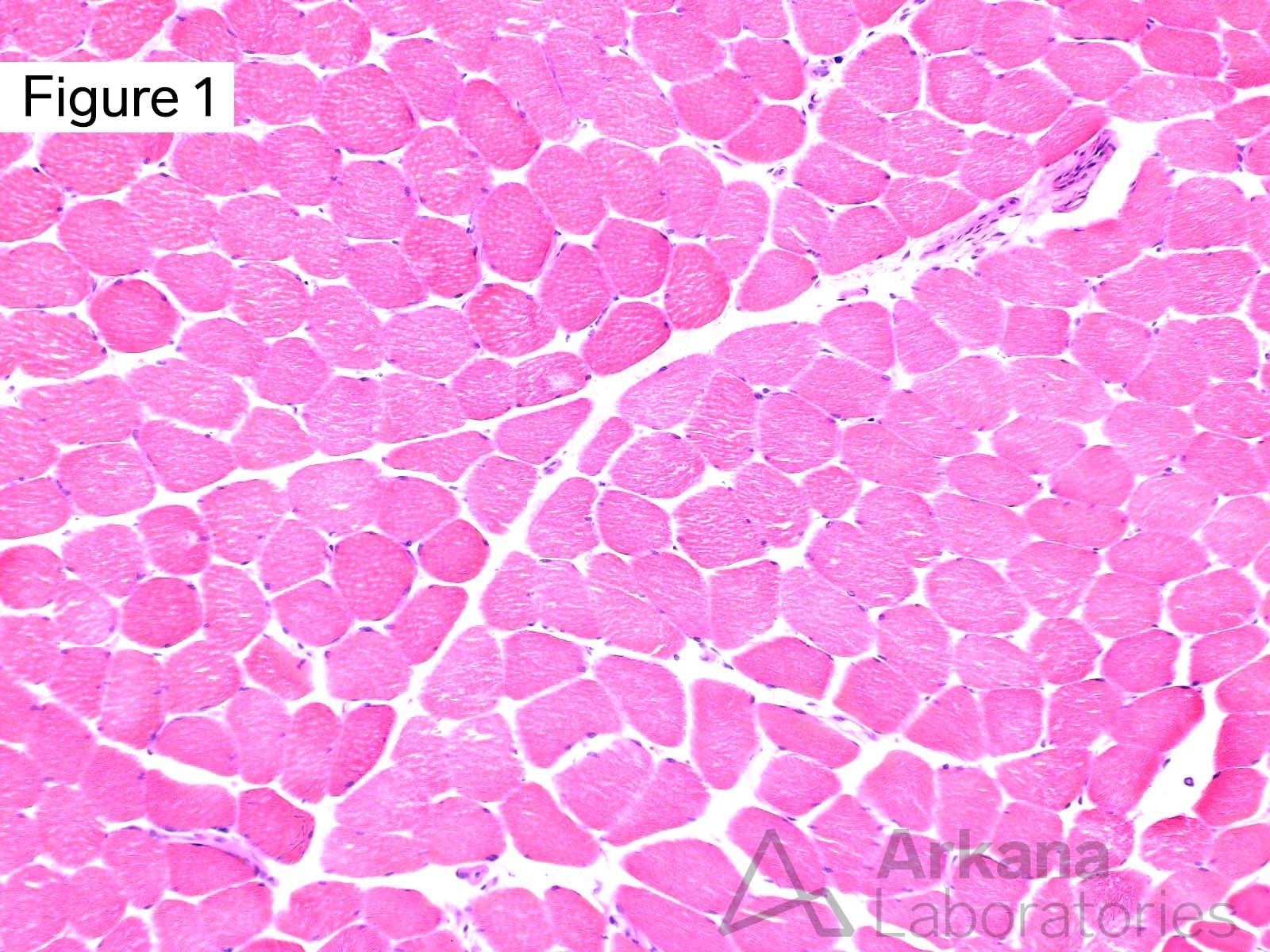
The biopsy tissue is well-preserved and the muscle fibers show mild variation in least mean diameter due to the presence of a few scattered acutely angulated atrophic myofibers. No inflammation or morphologic evidence of vasculitis is seen. No basophilic regenerating muscle fibers or necrotic muscle fibers are present. No perifascicular atrophy is noted.
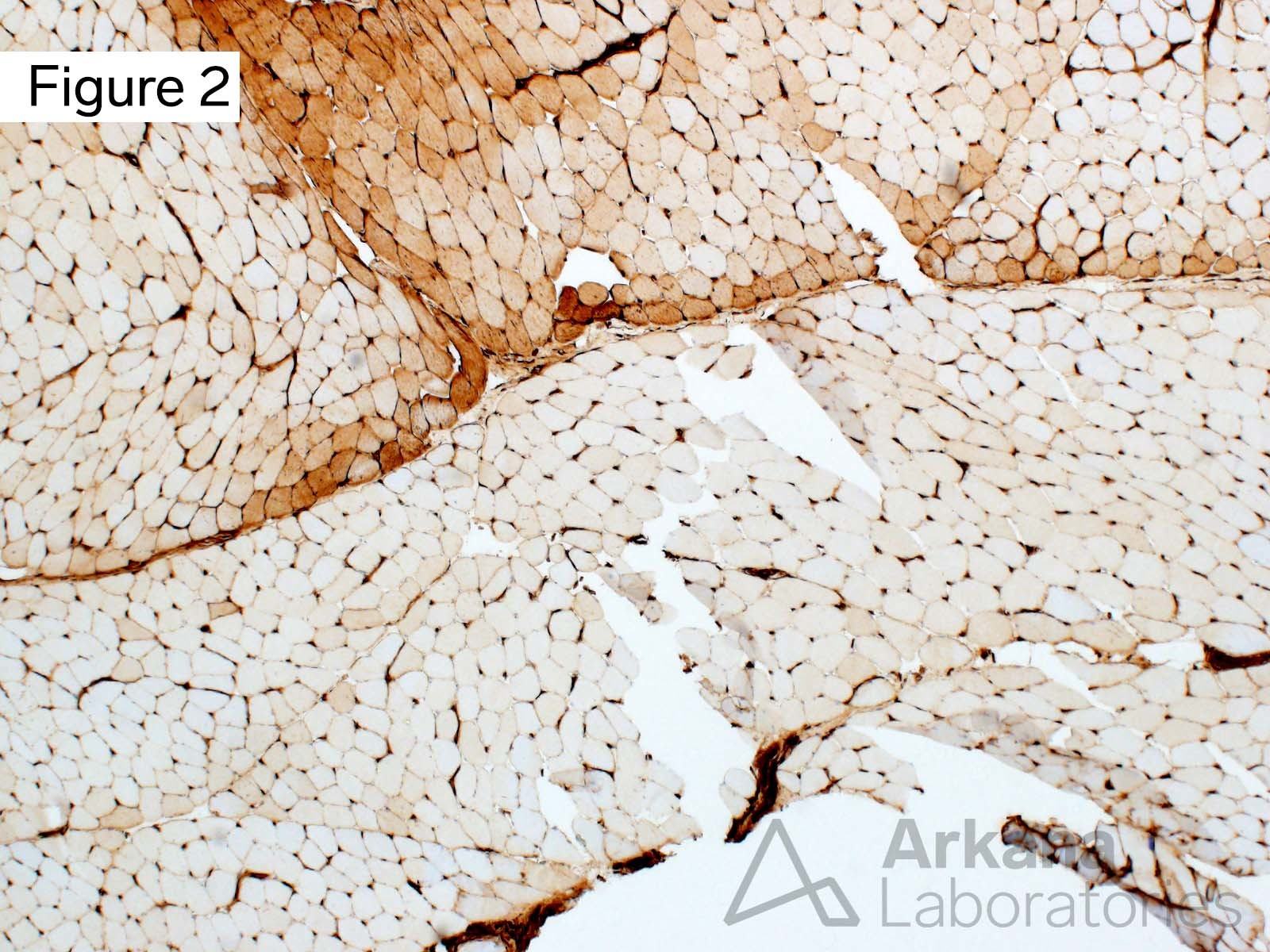
Note the presence of increased muscle fiber staining for MHC1 in a patchy perifascicular distribution (see arrows).
Answer: Treated dermatomyositis
The morphologic features seen on the H&E stained section are mild in degree and not specific. However, in the context of the patient’s clinical history (clinical features of dermatomyositis, positive NXP2 and TIF1-gamma autoantibodies, treatment prior to muscle biopsy), the finding of a perifascicular pattern of MHC1 staining is compatible with the presence of treated dermatomyositis.
This case is an example of the utility of performing stains other than H&E and modified Gomori Trichrome in the evaluation of muscle biopsies.
Features characteristic of polymyositis or necrotizing myopathy are not present. The biopsy tissue is well-preserved and the MHC1 staining is felt to not represent an artifact of partial tissue degradation.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.