Clinical History:
History: 68-year-old man with 1 week of bilateral proximal upper and lower extremity weakness and 1 month of facial, eyebrow, neck, chest, and back rash (initially diagnosed as seborrheic dermatitis).
PMH: HTN, PVD, asthma, hyperlipidemia, GERD, type 1 DM with retinopathy, IgA deficiency, hypothyroidism, former light smoker.
FH: Stroke, diabetes, arthritis, cancer, macular degeneration, heart disease.
Meds: Atorvastatin, insulin, levothyroxine, zolpidem; treated with Solu-Medrol and prednisone.
Physical exam: Mild-moderate proximal weakness, lower extremity edema.
MRI: Diffuse heterogeneous edema of bilateral quadriceps, adductors, and sartorius, suspicious for inflammatory myopathy.
Labs: CK peaked at 1570, trending down to 680; aldolase 20; mildly elevated CRP; ANA, Lyme, and RF negative; HMGCR Ab, MG panel, extended myositis and ENA panels pending.’
What is the primary etiology in this muscle based on this histology alone?
A. Myopathic
B. Dystrophic
C. Neurogenic
D. Inflammatory
Answer:
C. Neurogenic
Chronic active neurogenic changes
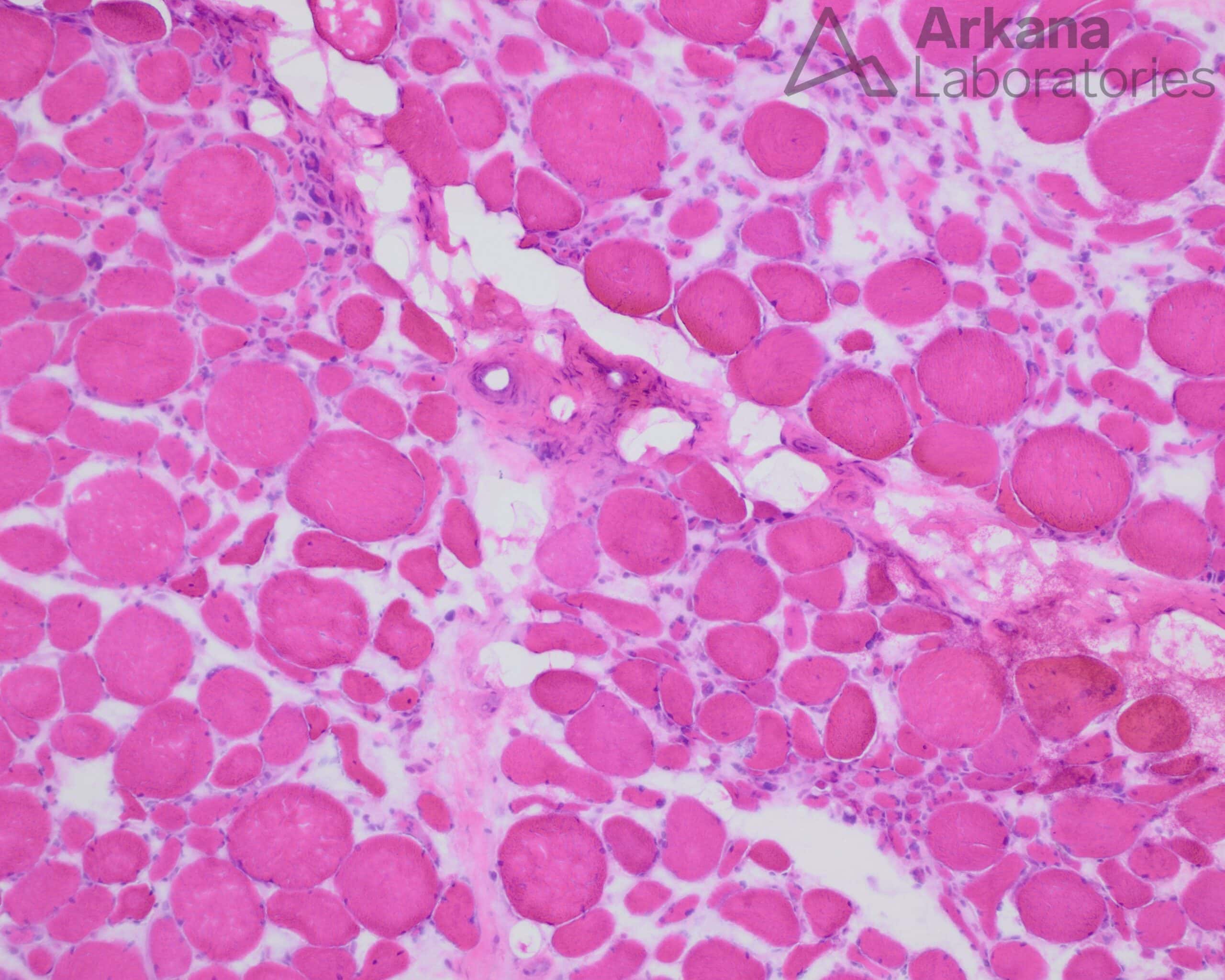
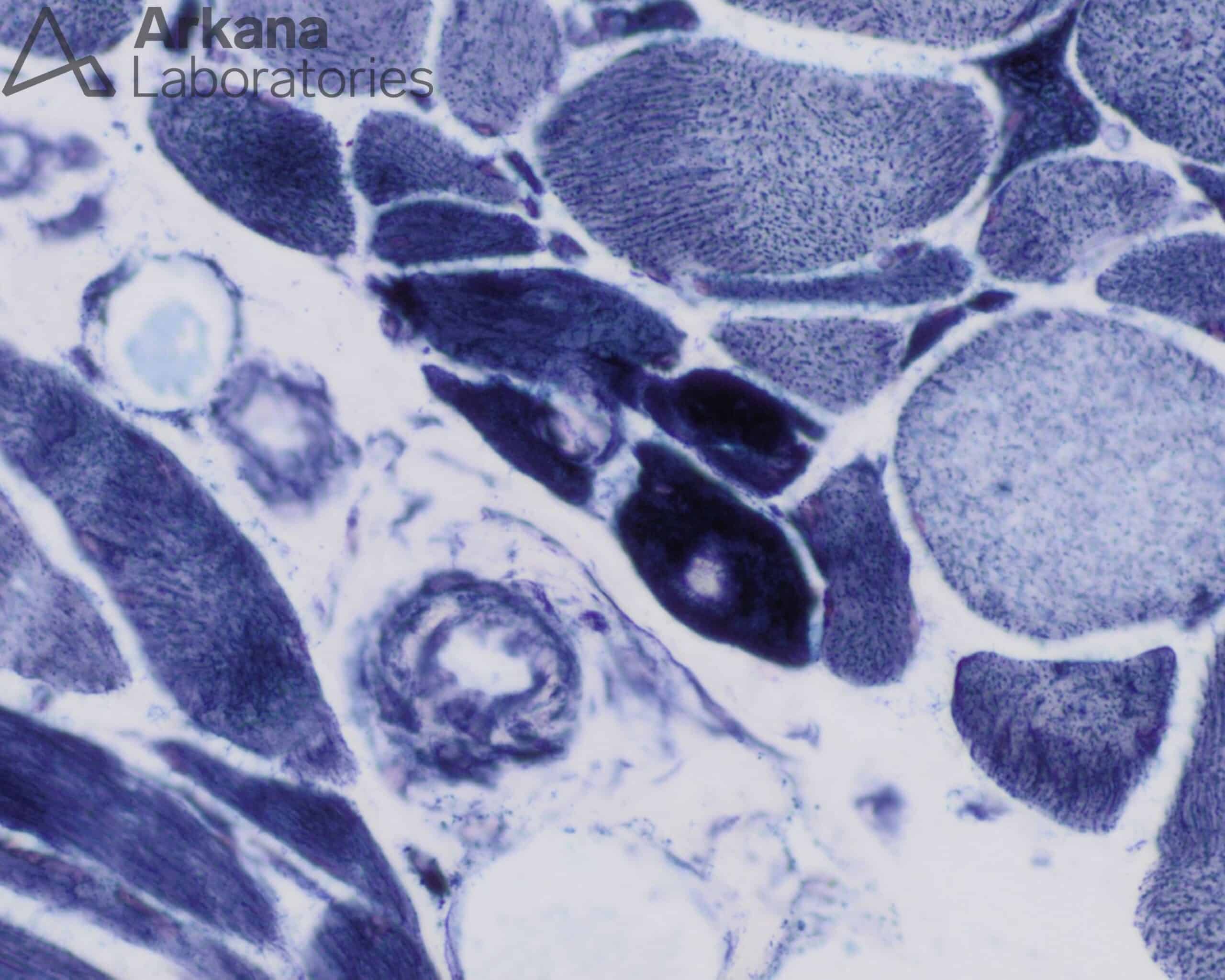
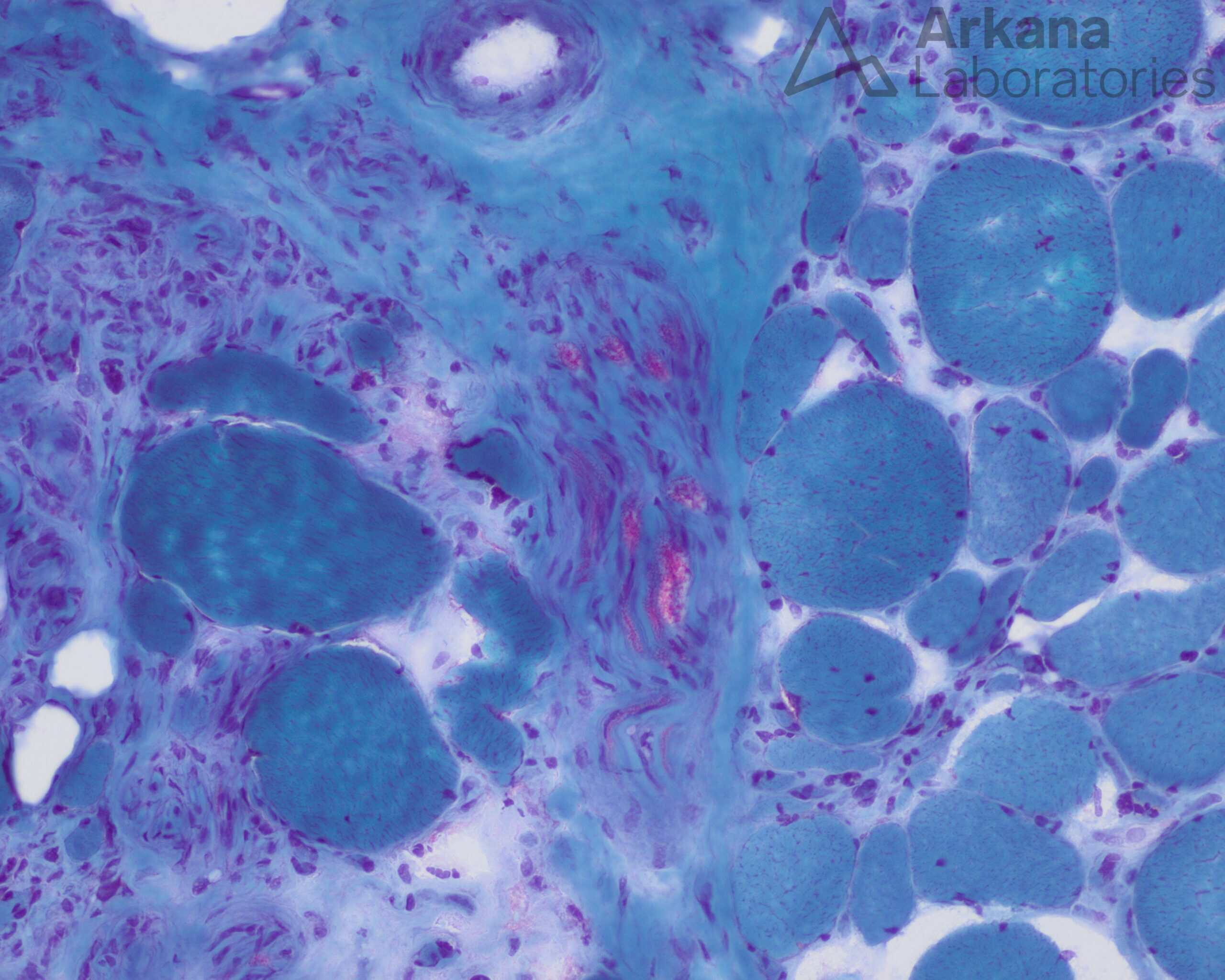
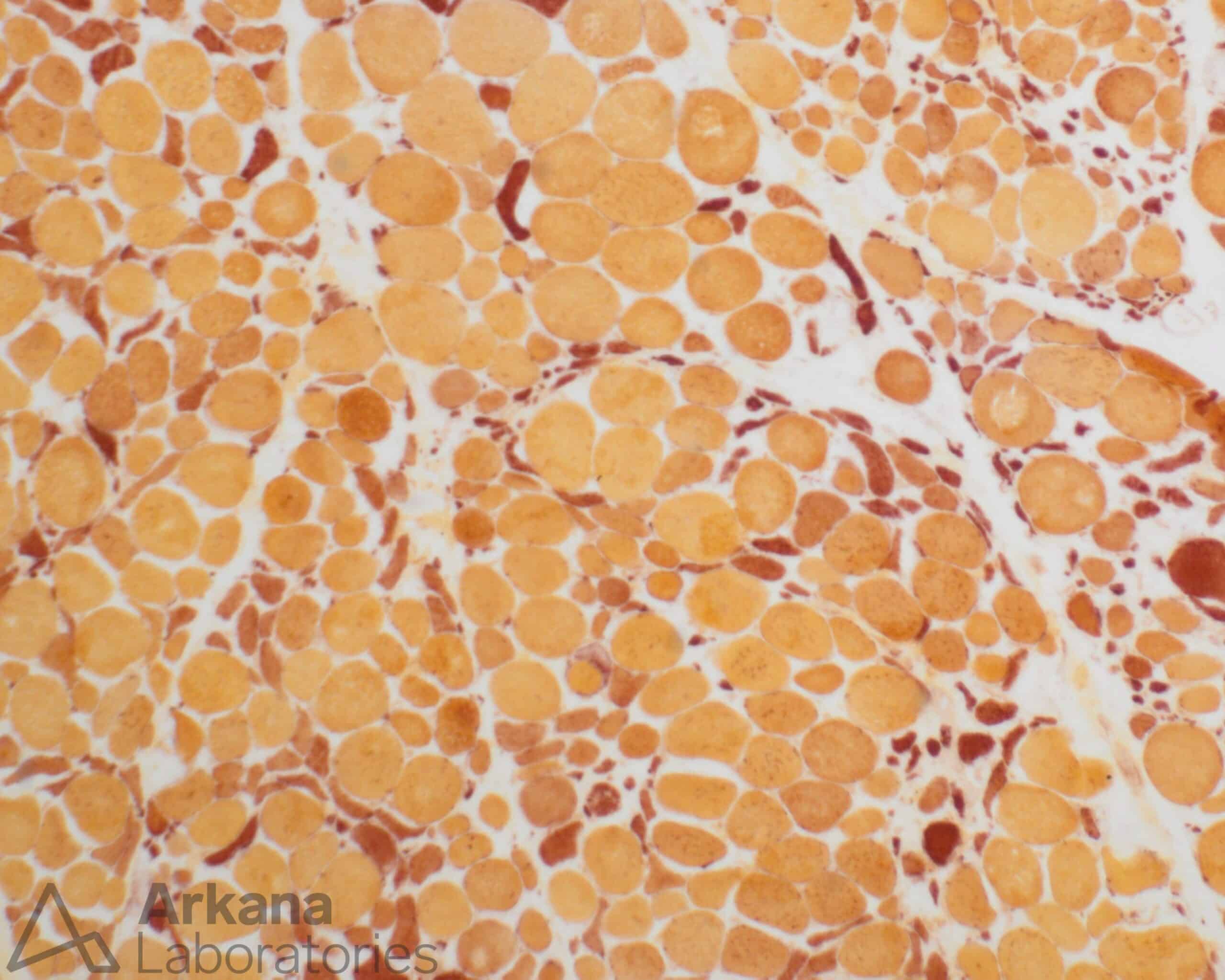
The findings in this muscle that are characteristic for active neurogenic changes are:
- Angulated atrophic fibers that stain darkly on esterase, along with nuclear bags.
- There is also a characteristic “Target” fiber with a light center surrounded by darker staining.
- The trichrome also reveals a peripheral nerve that appears partially depopulated of myelinated axons (red staining).
There is no necrosis, regeneration, fibrosis or internalized nuclei to suggest a myopathic process. Dystrophic muscle would show similar myopathic findings along with marked variation in fiber size and hypertrophic fibers with splitting. An inflammatory processes would most likely be characterized by the presence lymphocytes.
Common etiologies:
- Motor nerve injury of any cause (trauma, diabetes, toxins, alcohol, and compression including radiculopathy, etc.)
- Peripheral motor neuropathy including inflammatory (e.g. “axonal” Guillain-Barre syndrome/acute motor axonal neuropathy)
- Vasculitis
- Inherited neuropathies (e.g. Charcot-Marie-Tooth disease)
- Motor neuron disease, myelopathy
- Multiple sclerosis
- CNS ischemic vascular disease
Reference(s) / Additional Reading:
- Biopsy Diagnosis of Peripheral Neuropathy, 2nd Edition. JM Bilbao and RE Schmidt, eds. Springer, New York. 1995, 484 pp.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.