Clinical History:
This 50-year-old patient presented with progressively worsening muscle weakness of one month duration. Their past medical history was significant for type 2 diabetes, hyperlipidemia, hypertension and hypothyroidism. Statin medication (atorvastatin) was held upon admission. The patient’s home medication list included levothyroxine. They were treated with steroid prior to muscle biopsy.
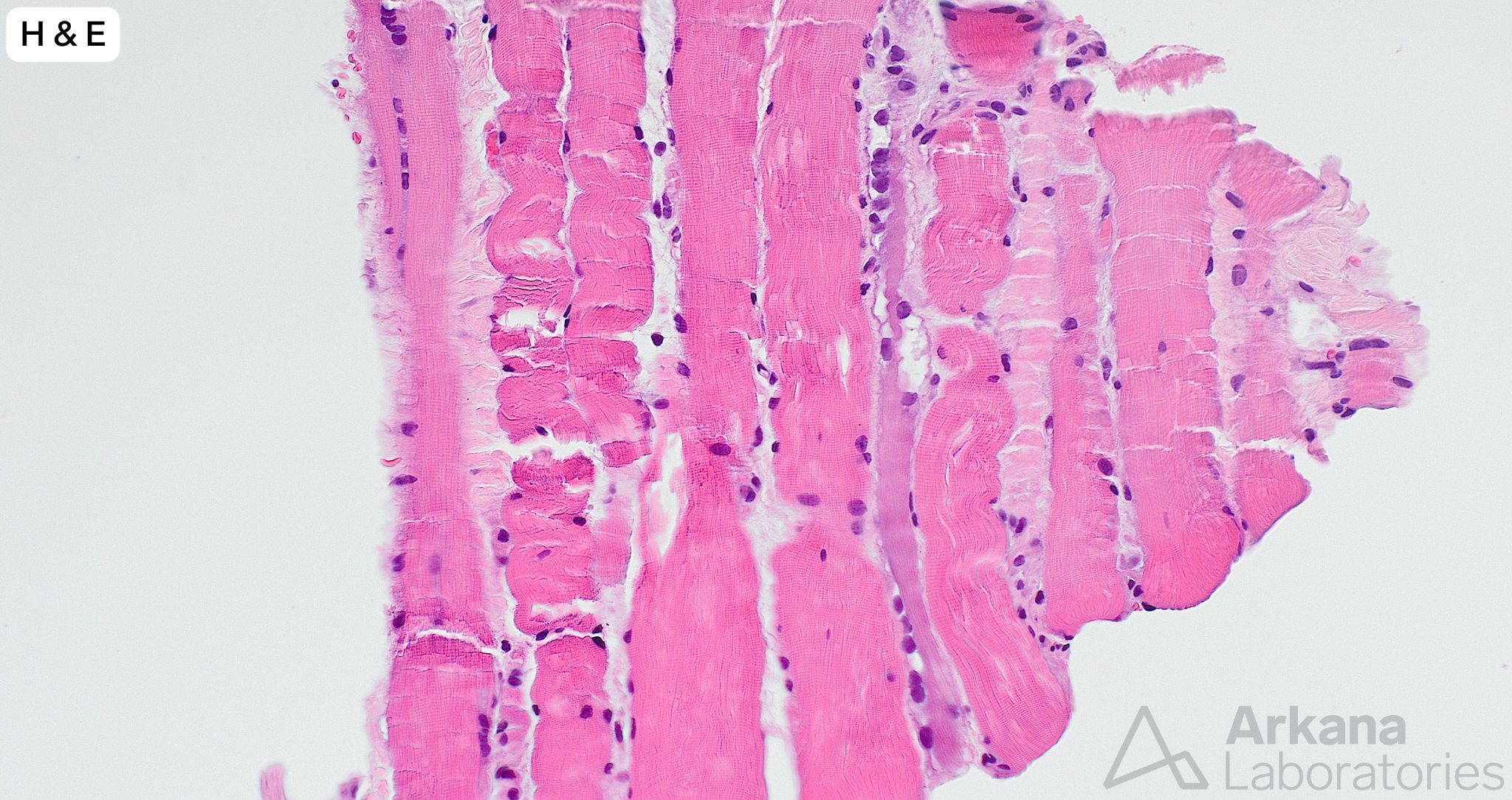
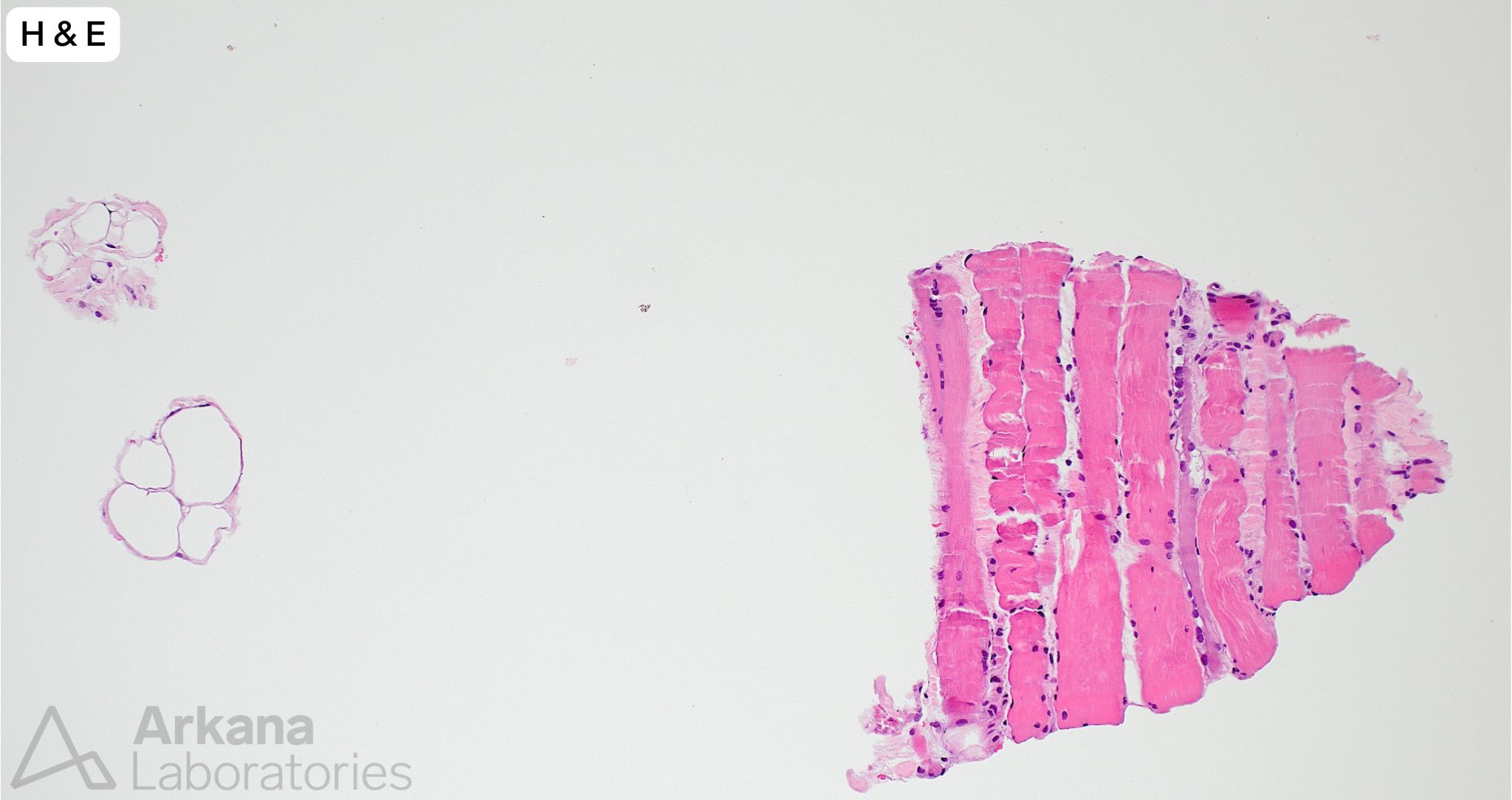
A needle core biopsy was performed of the left thigh. A minute fragment of fibrous tissue was present in tissue available for frozen section. The provided images (low and high magnification) show the total tissue available for evaluation in the formalin-fixed paraffin embedded tissue. The tiny fragment of glutaraldehyde-fixed tissue available for toluidine blue stained sections (image not provided) showed features similar to those seen in the FFPE tissue sections, and a few necrotic myofibers.
What is the best pathologic diagnosis?
A. Inclusion Body Myositis
B. Necrotizing Myopathy
C. Vasculitis
D. Normal Muscle
Answer:
Necrotizing Myopathy
- The amount of tissue is extremely limited but shows a few regenerating and necrotic myofibers without associated chronic lymphoid inflammation. The overall changes are best categorized under the nonspecific descriptive umbrella term “necrotizing myopathy.”
- The pathologic alterations of necrotizing myopathy are not entirely specific as to etiology as they may be seen in a variety of contexts, including toxic myopathy (for example statin medication), immune-mediated necrotizing myopathy (SRP and HMGCR autoantibodies), partially treated acquired inflammatory myopathy, paraneoplastic myopathy, endocrine myopathy (thyroid), metabolic myopathy and infectious myopathy (viral).
- While significant information may be obtained from needle core biopsy samples, the “risk” of an issue of sampling compared to open biopsy is accentuated (i.e. processes involving muscle are frequently patchy in nature and morphologic features to enable a definitive pathologic diagnosis may be only partially represented or not present at all in the tissue submitted for evaluation).
- Morphologic features diagnostic for Inclusion Body Myositis of vasculitis are not present in the tissue available for evaluation. But both of these entities may focally show features similar to those seen in the submitted sample.
- The number of needle core (16 gauge) biopsies of muscle we receive for evaluation is increasing. While significant information may obtained from such samples, their limitations must be understood. Needle core biopsy of a patient with suspected metabolic myopathy would be inappropriate.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.