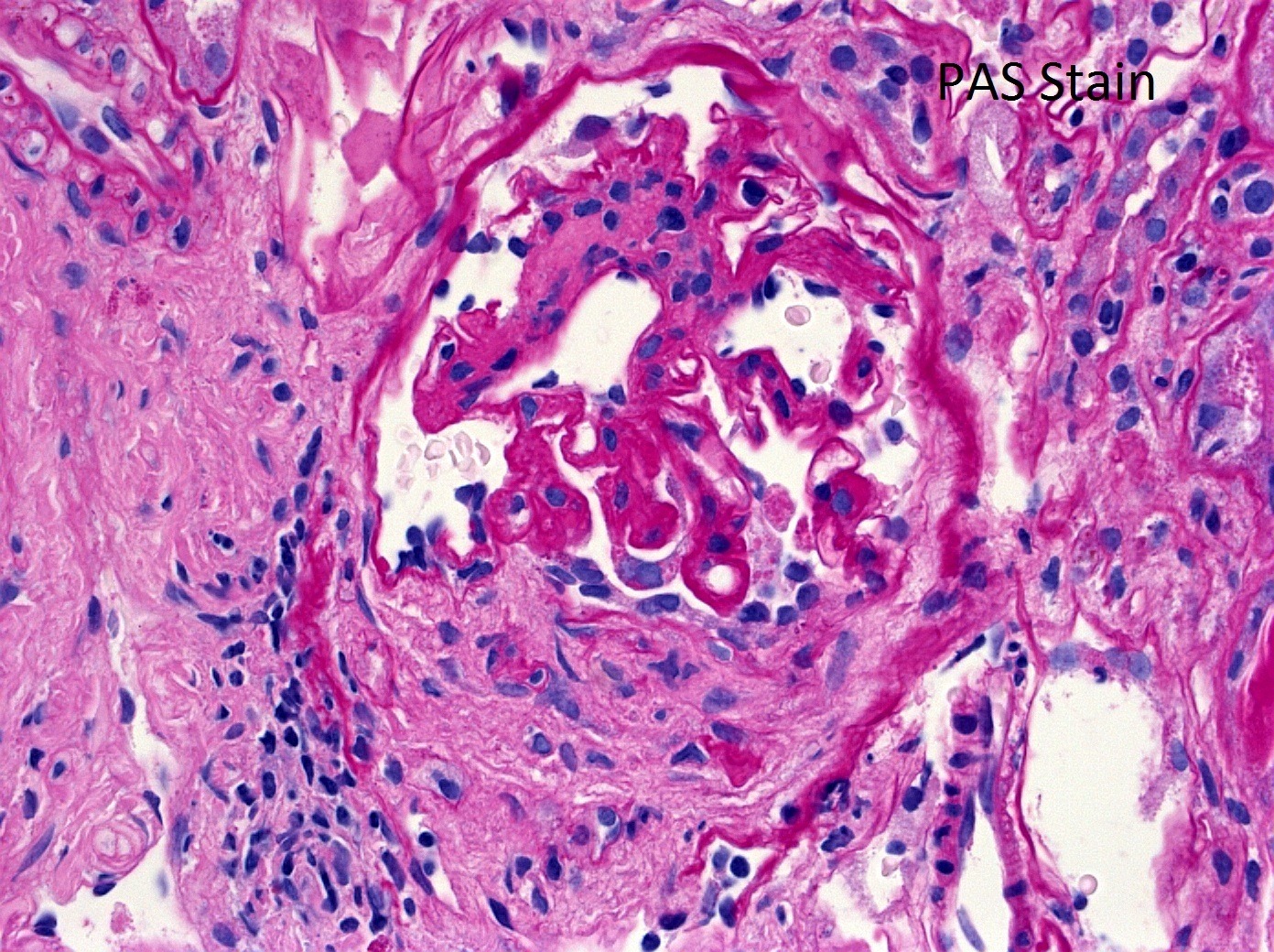
The patient is a 30-year-old female who presents with nephrotic range proteinuria and a creatinine of 2.5. She has a history of hypertension and joint pains. Serologies for ANA, dsDNA, and ANCA are negative.
What is the best diagnosis?
A. ANCA-associated Glomerulonephritis
B. C3 Glomerulonephritis
C. Membranous-like Glomerulopathy with Masked IgG Kappa Deposits
D. Proliferative Glomerulonephritis with Monoclonal IgG Kappa Deposits
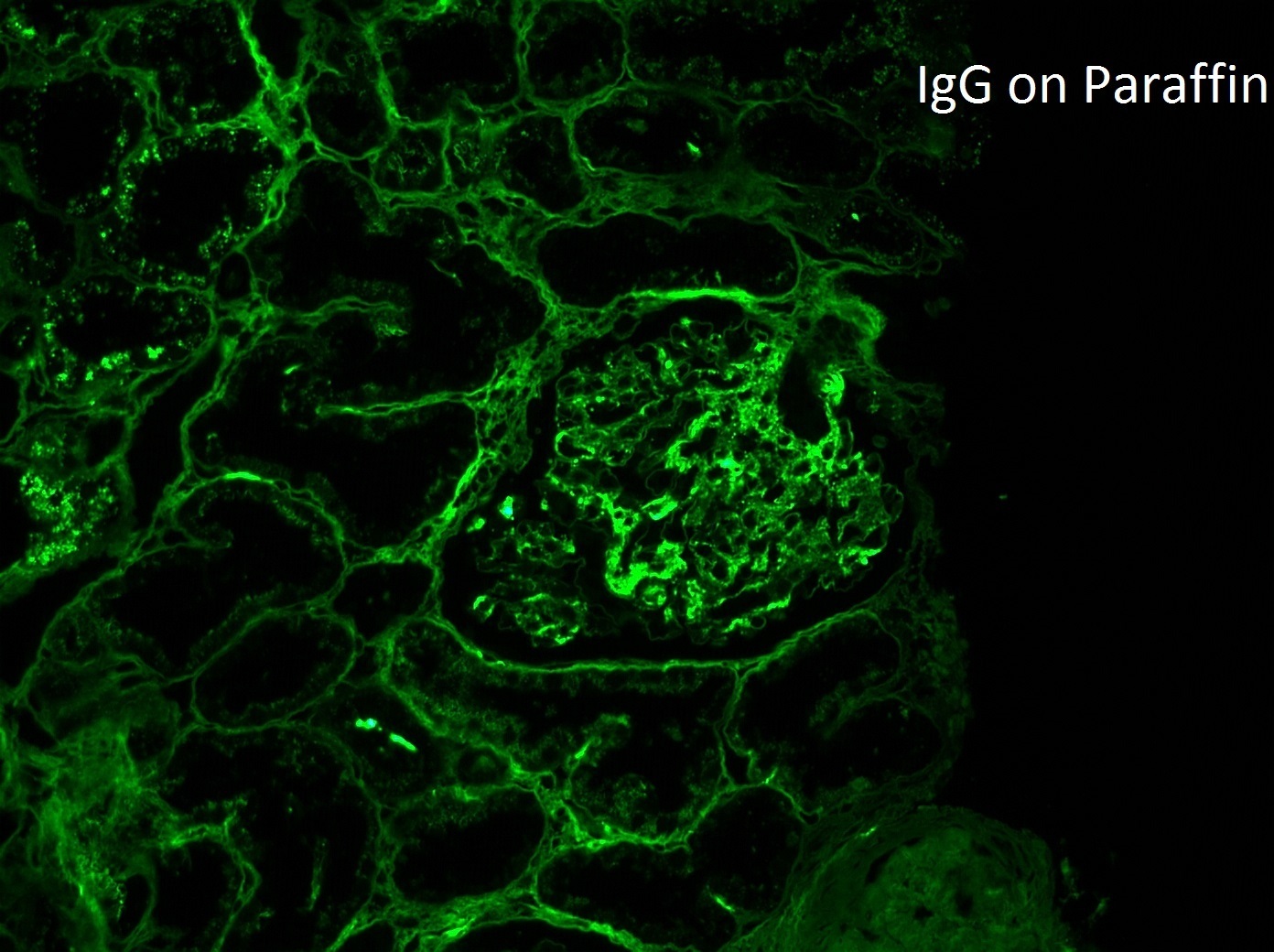
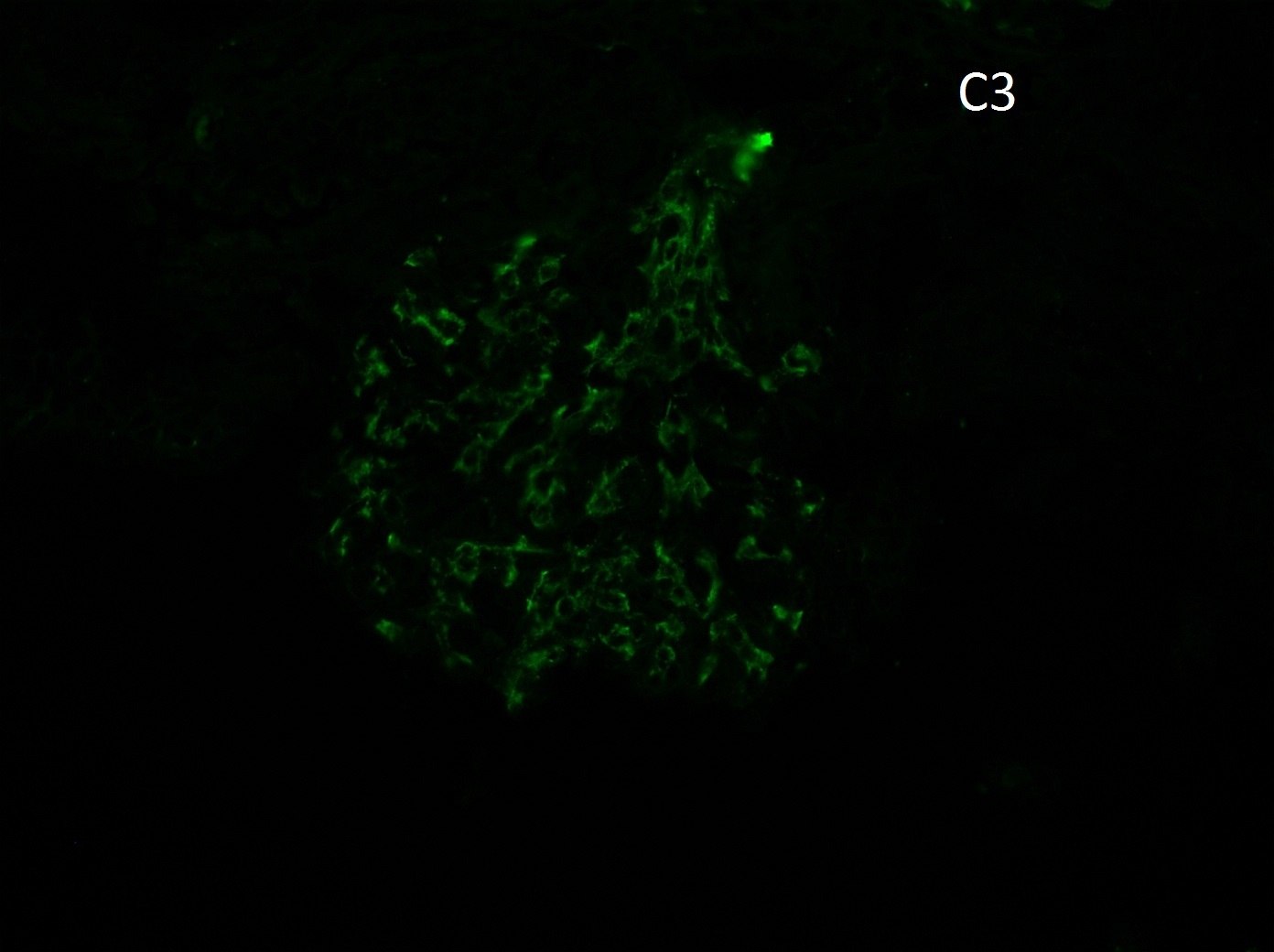
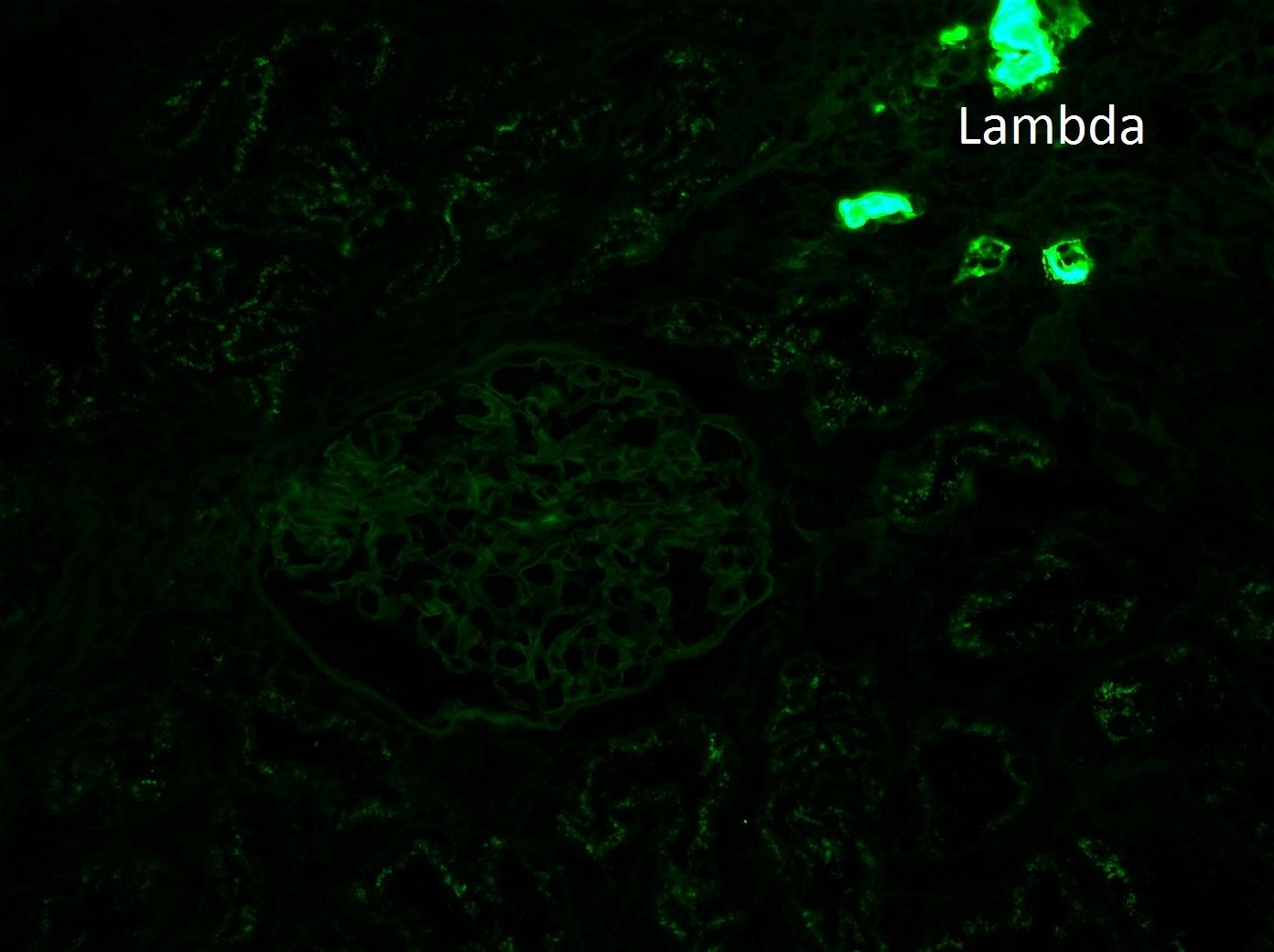
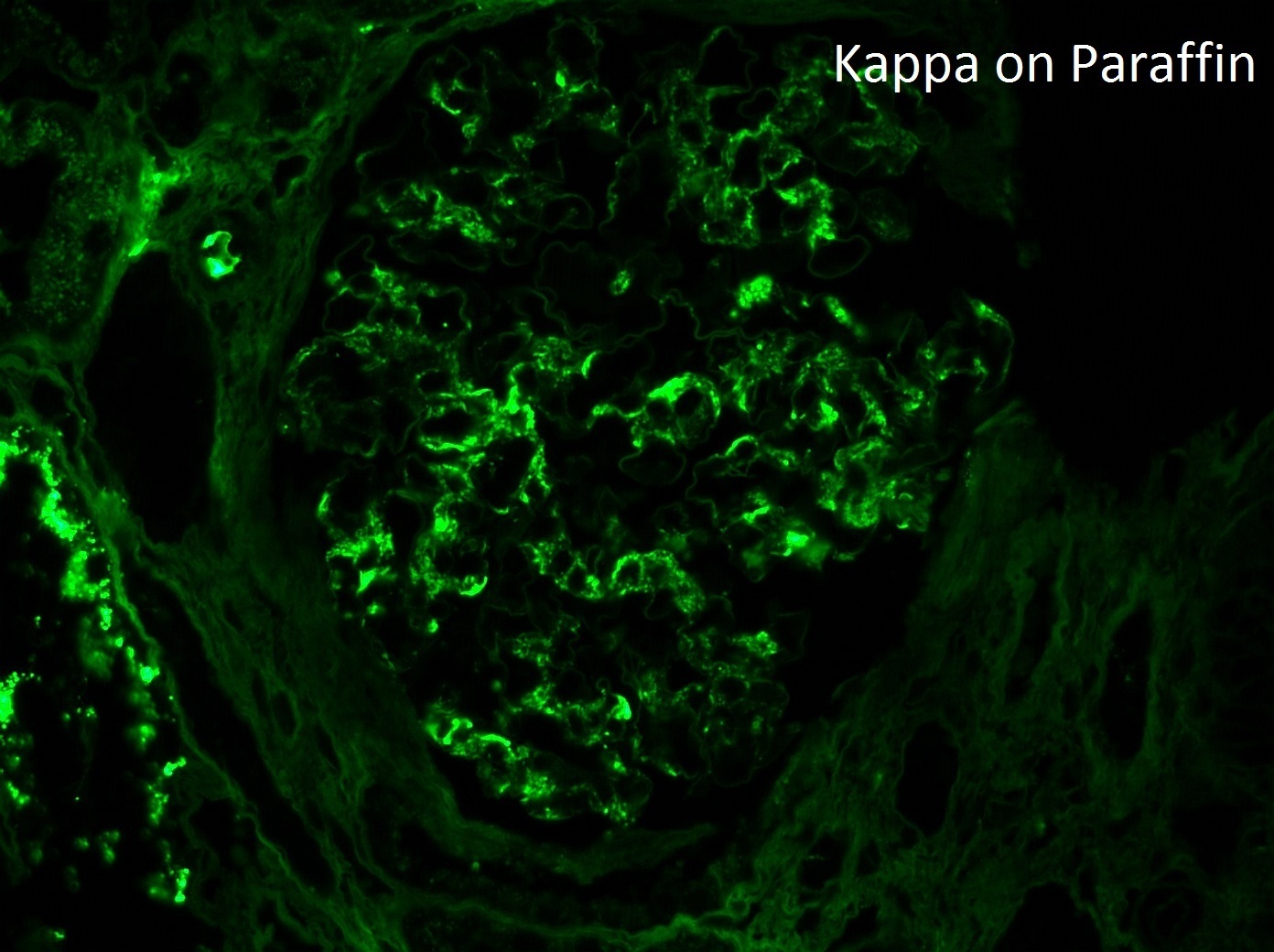
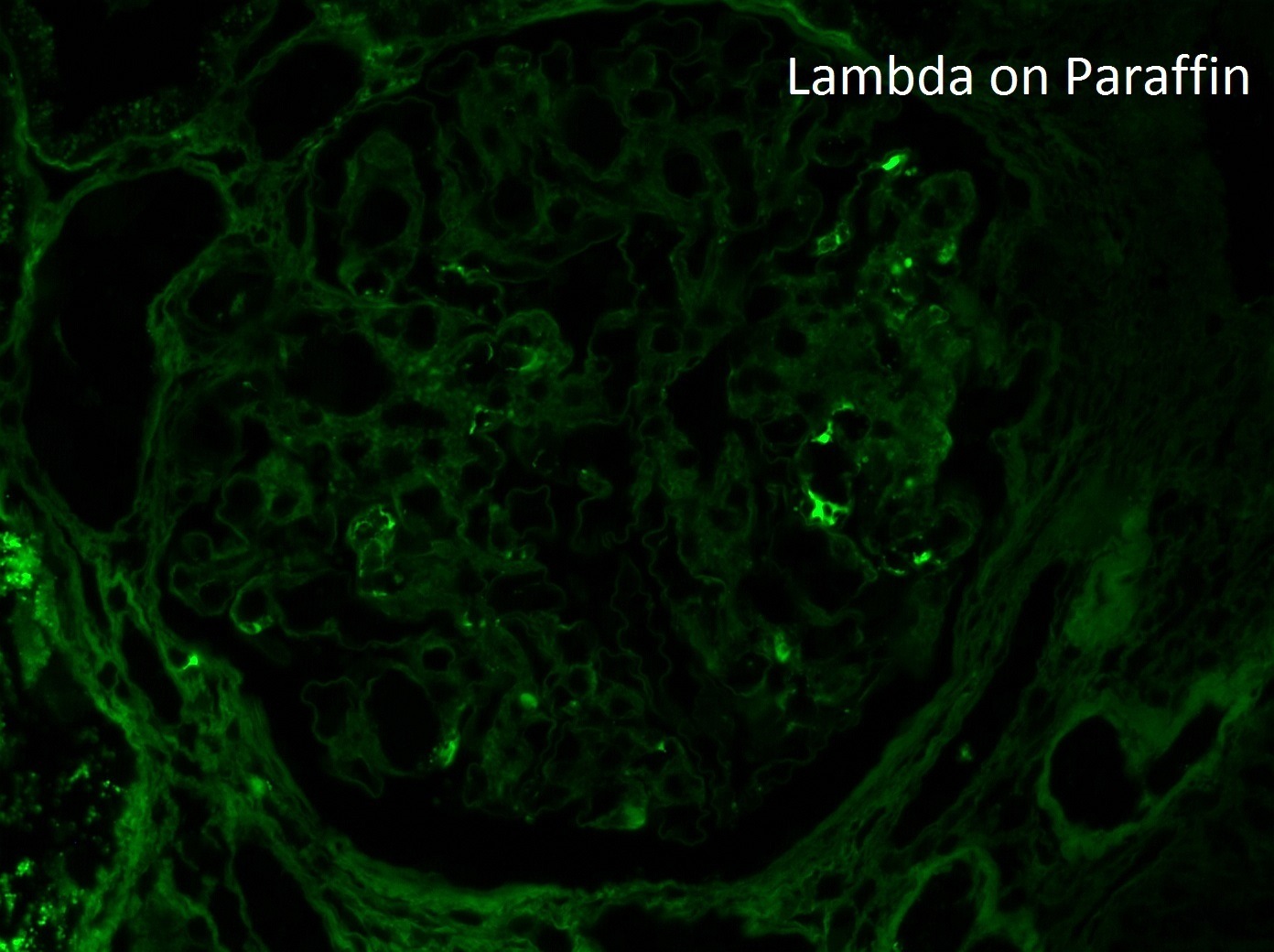
The best answer is C: Membranous-like Glomerulopathy with Masked IgG Kappa Deposits.
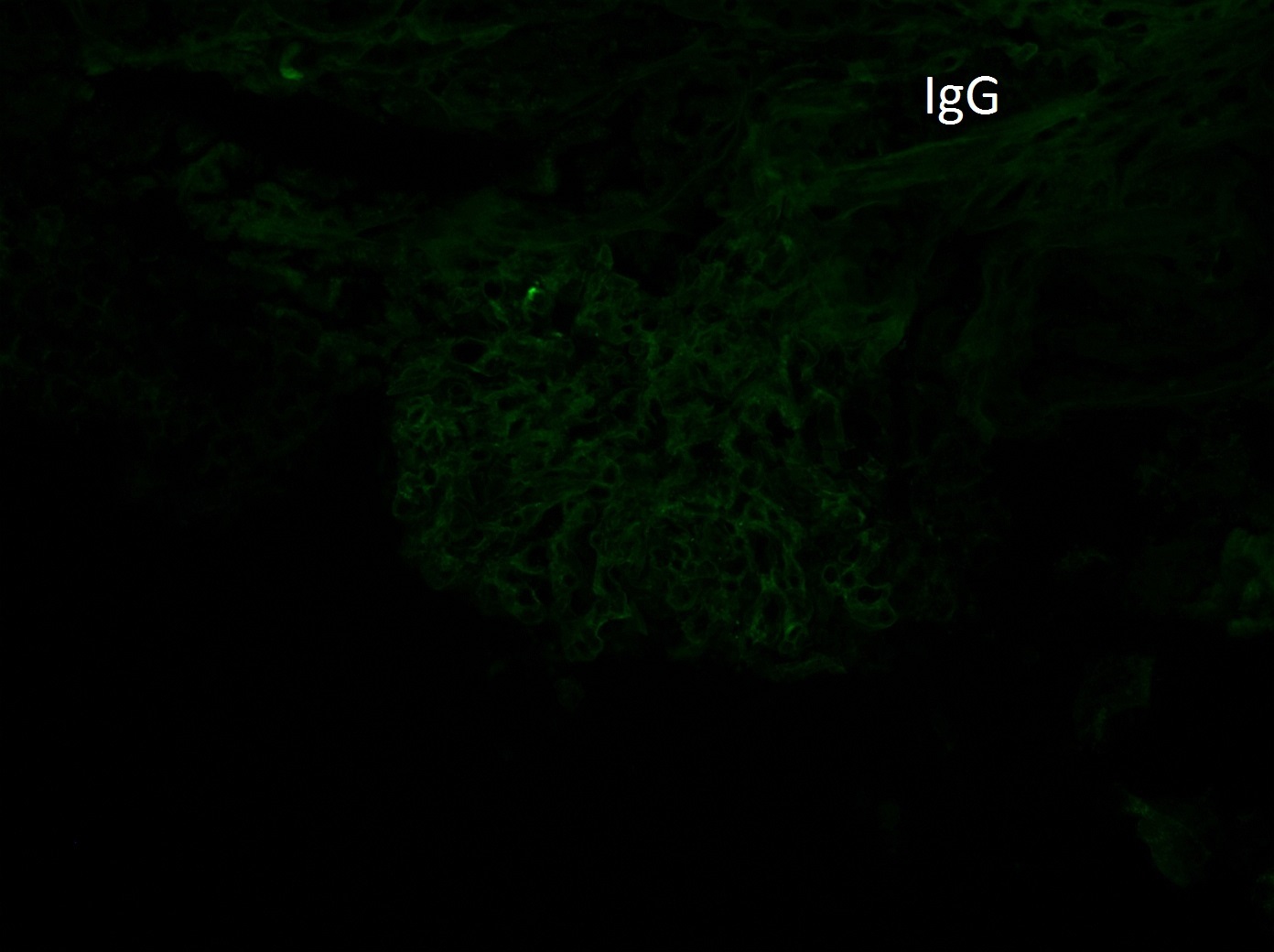
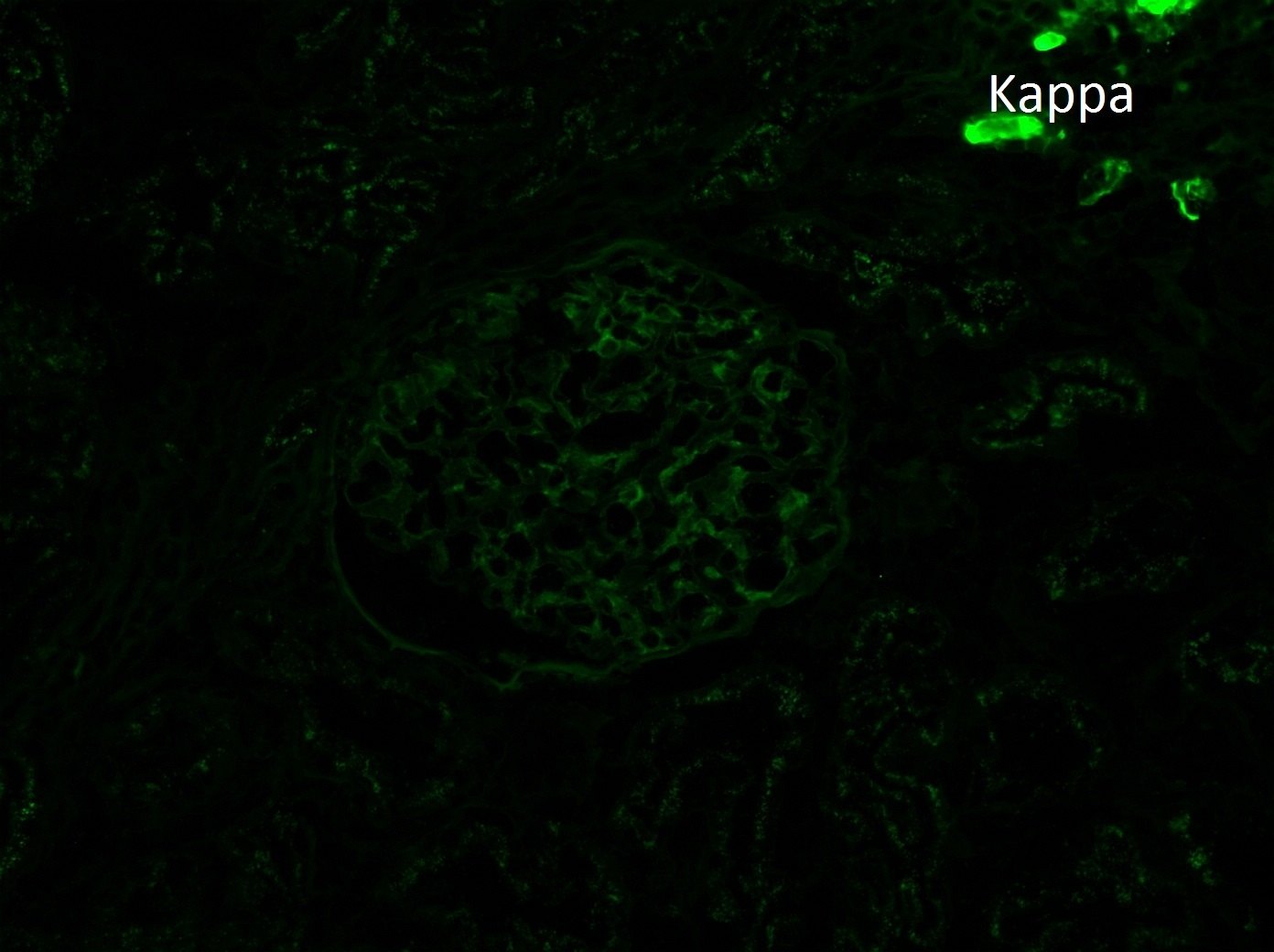
An ANCA-associated glomerulonephritis is a possibility with the fibrous crescent and weak direct immunofluorescence staining. However, the ANCA is negative and the immunofluorescence stains are “unmasked” on the paraffin-embedded tissue. C3 glomerulonephritis is sometimes misdiagnosed in cases of membranous-like glomerulopathy with masked IgG kappa deposits because the paraffin tissue is not tested to look for “masked” deposits. Proliferative glomerulonephritis with monoclonal IgG kappa deposits refers to a glomerulonephritis which stains for IgG, C3, and kappa by direct immunofluorescence. In this case, the IgG and kappa were only “unmasked” on the paraffin-embedded tissue. For further reading, please follow this link https://www.ncbi.nlm.nih.gov/pubmed/24429395
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.