Clinical presentation
A 49-year-old male presents with acute deterioration in renal function. The serum creatinine is 4.5 mg/dL. He has been receiving methotrexate for osteosarcoma.
Kidney biopsy findings
Figures 1 and 2 (H&E stain) show the main findings on kidney biopsy.
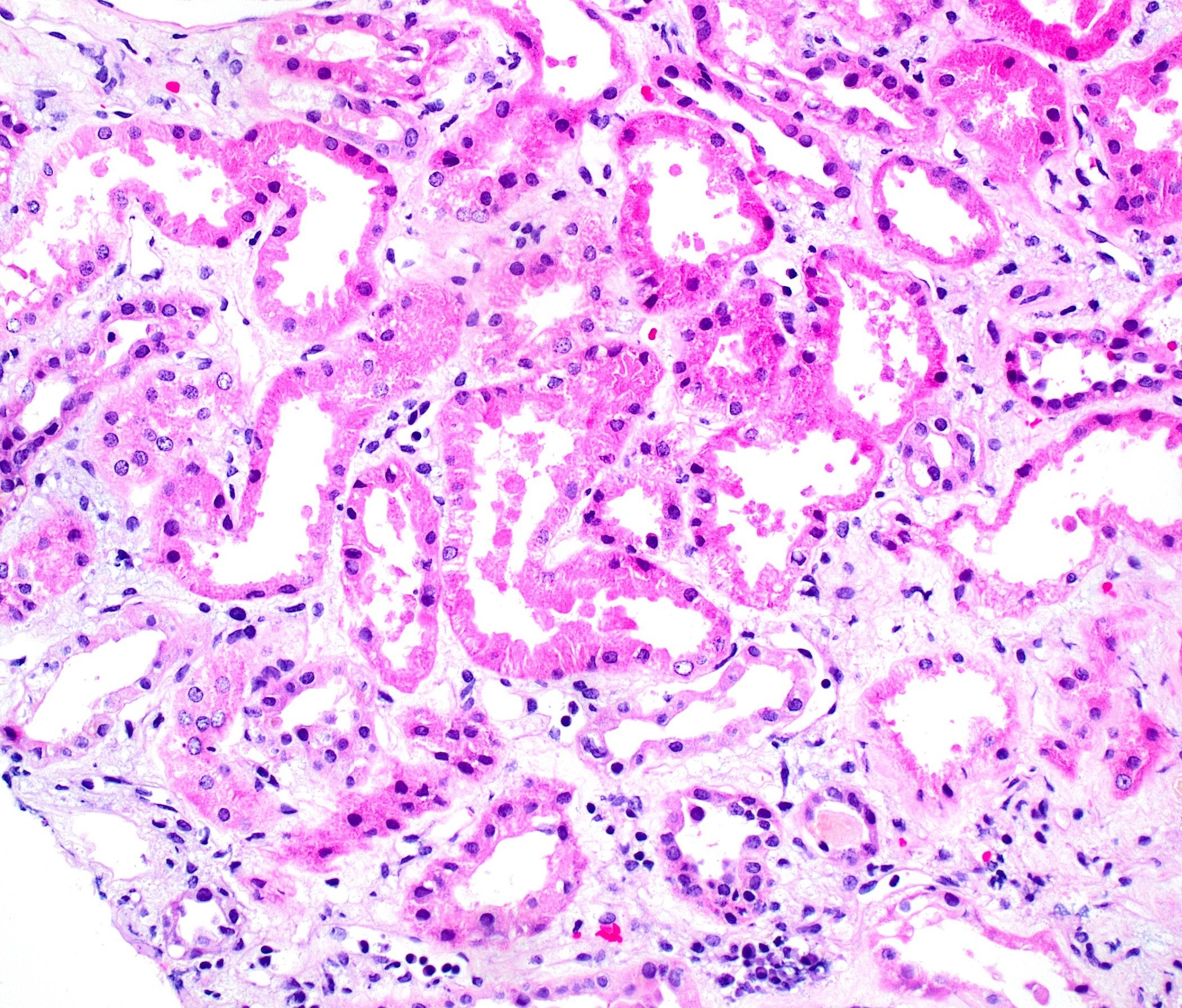
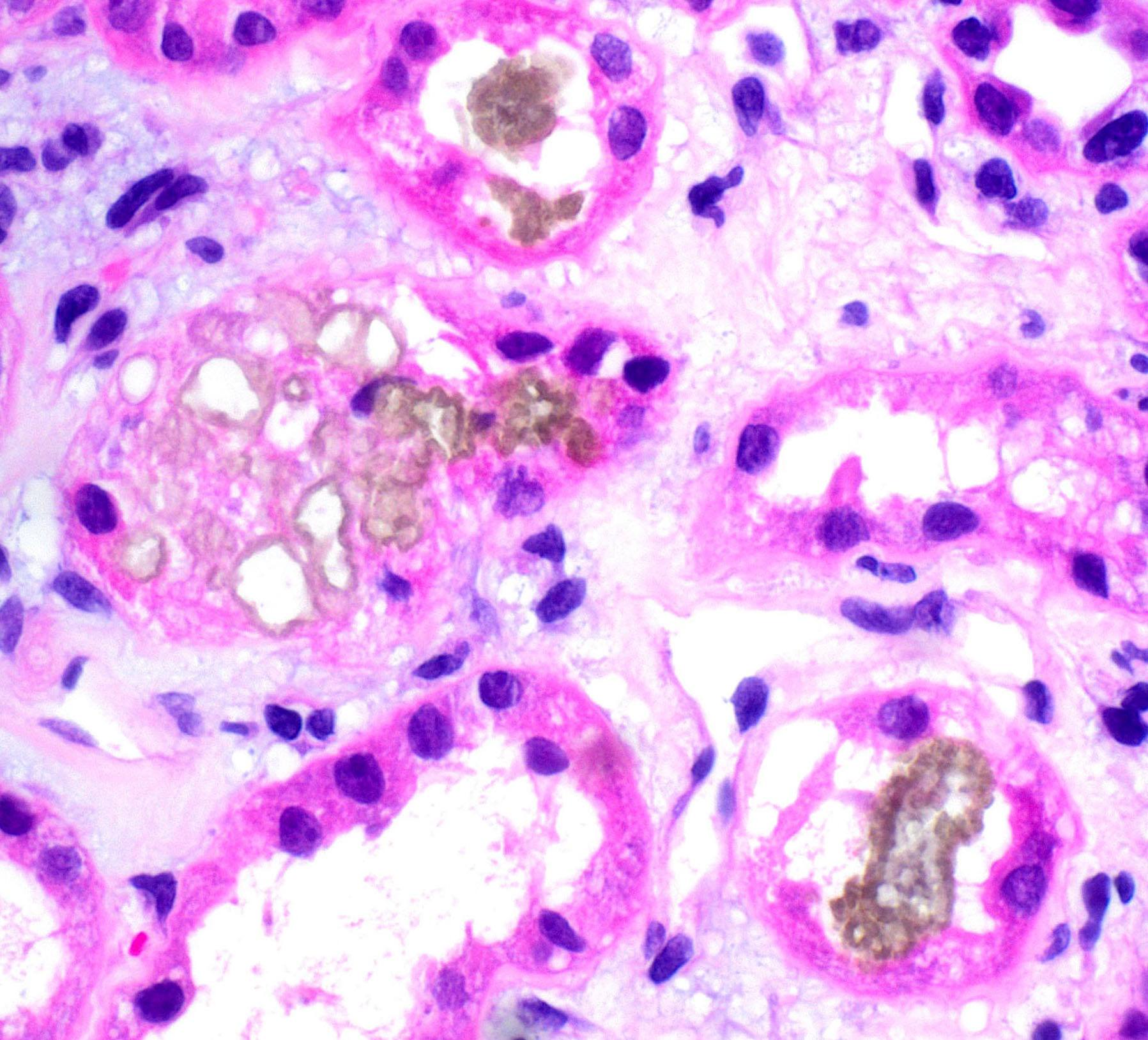
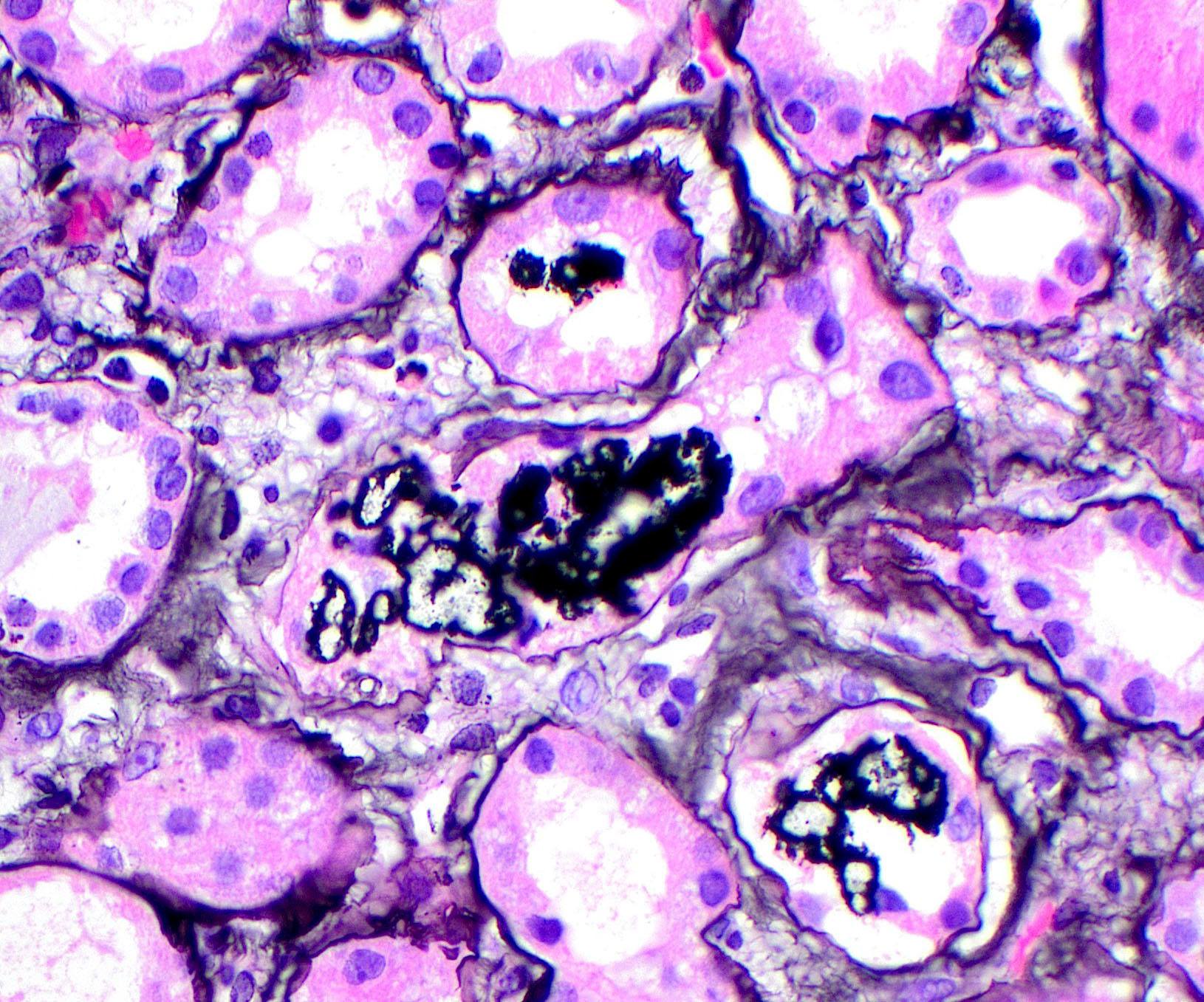
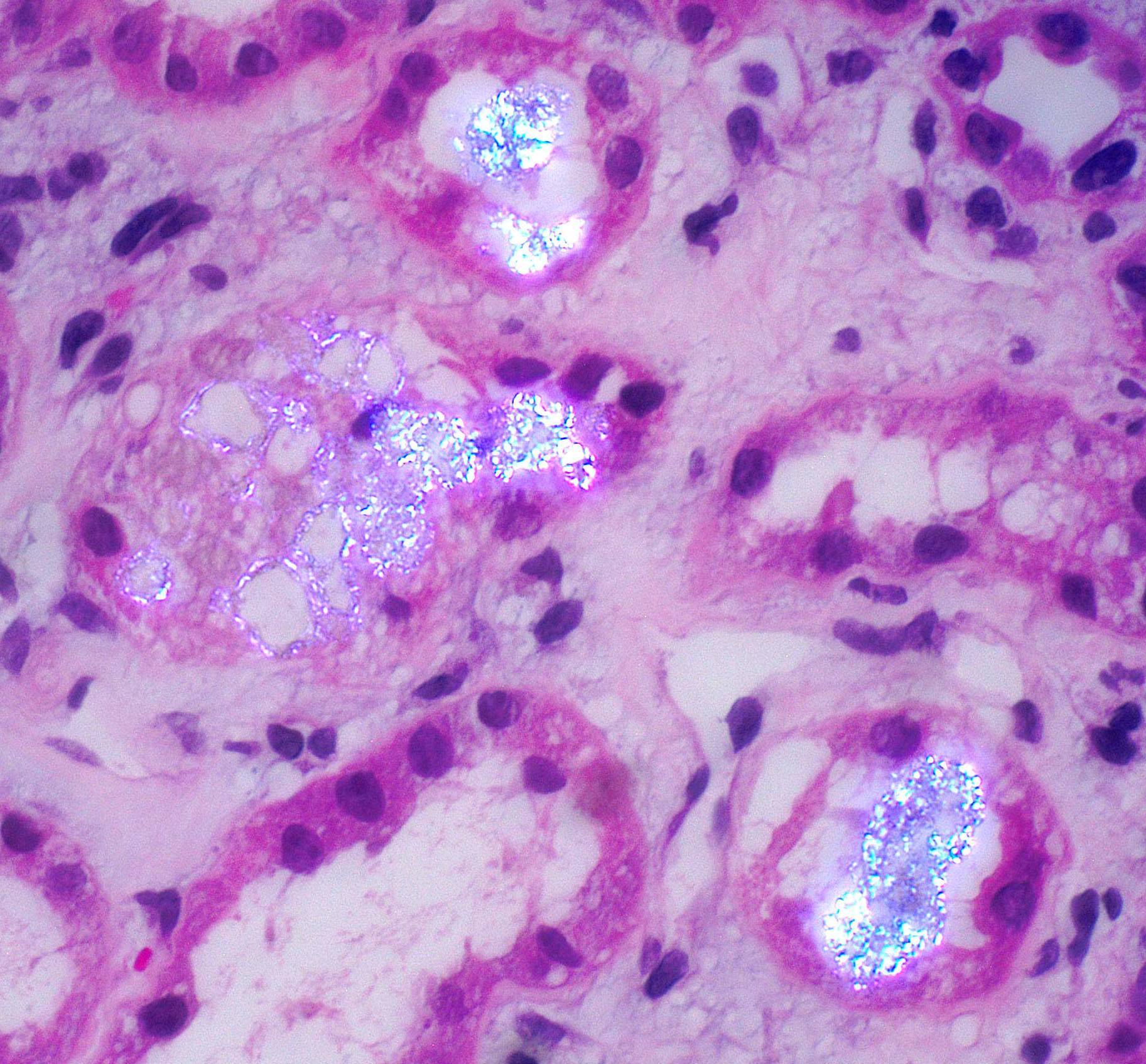
In Figure 1, the tubular epithelium shows features of acute injury such as attenuation, dilatation, and reparative changes. Note the background interstitial edema. Figure 2 shows yellow-brown crystals within tubular lumens. The crystals form annular structures, are silver positive (Figure 3), and strongly birefringent under polarized light (Figure 4).
Differential diagnosis
The finding of yellow to brown crystals on H&E stain that show strong birefringence under polarized light and stain silver positive raises three etiologic possibilities: 2,8 dihydroxyadeniuria (DHA), Methotrexate, and Triamterene. The shape and structure of the crystals can help in differentiating the etiology. However, review of the patient’s history and medication list is required.
| Shape | Silver stain | |
| 2,8 dihydroxyadeniuria (DHA) | Crystals form fan-like or irregular shapes | Positive black staining |
| Methotrexate | Small needle-shaped crystals that form annular structures | Positive black staining |
| Triamterene | May show Maltese crosses under polarization | Positive black staining |
What is the diagnosis?
The history and histological findings make the diagnosis methotrexate-induced crystalline nephropathy. Drug-induced crystalline nephropathy is a rare cause of acute kidney injury due to stones and crystals, less than 1% of cases. Acute kidney injury results from precipitation of the medication in the tubules, leading to obstruction and tubular epithelial cell injury. Risk factors include hypovolemia, underlying kidney disease, drug dose, and changes in urinary pH that promote crystal precipitation. Methotrexate-induced crystalline nephropathy is most commonly seen in patients treated with high-dose methotrexate for solid tumors or hematologic malignancies.
References
Colvin, Robert, B. and Anthony Chang. Diagnostic Pathology: Kidney Diseases. Available from: Elsevier eBooks+, (3rd Edition). Elsevier – OHCE, 2019.
Cecyn KZ, Lee J, Oguro T, Petrilli AS, Bordin JO. Use of plasma exchange in methotrexate removal in a patient with osteosarcoma and acute renal insufficiency. Am J Hematol. 2003;72(3):209-211.
Jennette JC, Olson JL, Silva FG, D’Agati V, Heptinstall RH *1920 *, eds. Heptinstall’s Pathology of the Kidney: Includes Interactive EBook with Complete Content. Seventh edition. Wolters Kluwer; 2015.
Nicholas Cossey L, Dvanajscak Z, Larsen CP. A diagnostician’s field guide to crystalline nephropathies. Seminars in Diagnostic Pathology. 2020;37(3):135-142.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.