What is your diagnosis?
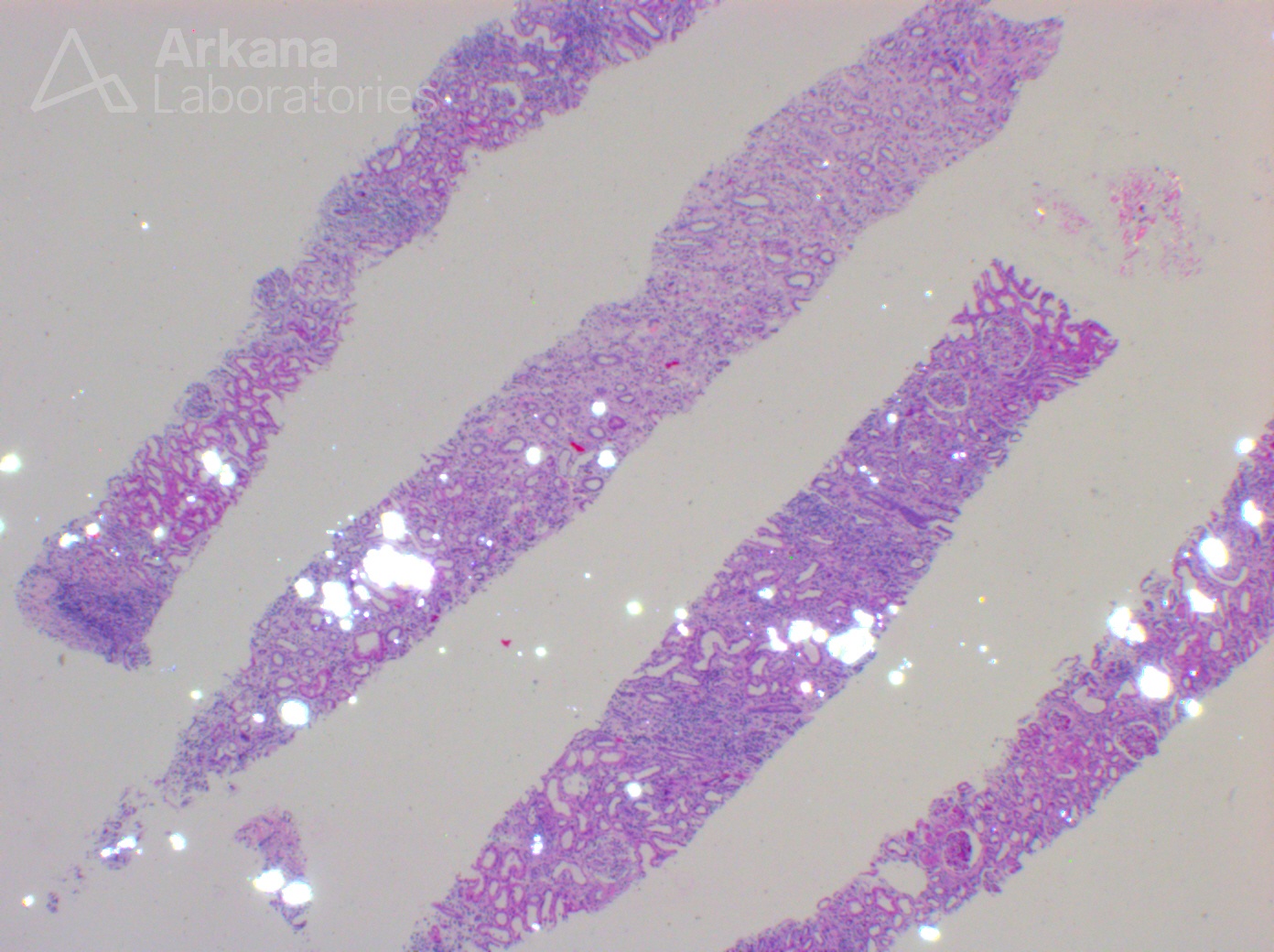
The image shows numerous intratubular crystals showing birefringence on polarization. The most common types of parenchymal crystals are calcium phosphate and calcium oxalate. Unlike calcium phosphate crystals that often show purple coloration and lack birefringence, calcium oxalate crystals are typically colorless but show strong birefringence on polarization. In the setting of CKD and acute tubular injury, it is not uncommon to see occasional intratubular calcium phosphate/oxalate crystals as these states provide environments that are more favorable to crystal nucleation. However, diffuse crystal formation is unusual and may represent nephrocalcinosis/renal oxalosis. The differential diagnosis for renal oxalosis is wide and includes primary hyperoxaluria, ethylene glycol intoxication, enteric hyperoxaluria (e.g. due to gastric bypass, chronic pancreatitis, small bowel resection, or malabsorption), vitamin B6 deficiency, excessive ingestion of vitamin C or dietary substances rich in oxalic acid (parsley, nuts, and star fruit, sweet tea, etc), and various drugs (e.g., methoxyflurane, Orlistat, Praxilene, COX-2 inhibitors), among others.
References:
Nasr S, D’Agati D, et al. Oxalate Nephropathy Complicating Roux-en-y Gastric Bypass: An Unrecognized Cause of Irreversible Renal Failure. Clin J Am Soc Nephrol 2008 Nov; 3(6):1676-1683.
https://www.ncbi.nlm.nih.gov/pubmed/18701613
Cossey LN, et al. Oxalate nephropathy and intravenous vitamin C. Am J Kid Dis 2013; 61:1032-1035.
https://www.ncbi.nlm.nih.gov/pubmed/23548555
Cartery C, Faguer S, Karras A, Cointault O, Buscail L, Modesto A, Ribes D, Rostaing L, Chauveau D, Giraud P. Oxalate nephropathy associated with chronic pancreatitis. Clin J Am Soc Nephrol. 2011 Aug;6(8):1895-902.”
https://www.ncbi.nlm.nih.gov/pubmed/21737848
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.