Immunofluorescence shows C3 (2-3+), IgM (1+), kappa (trace) and lambda (trace).
What is your diagnosis?
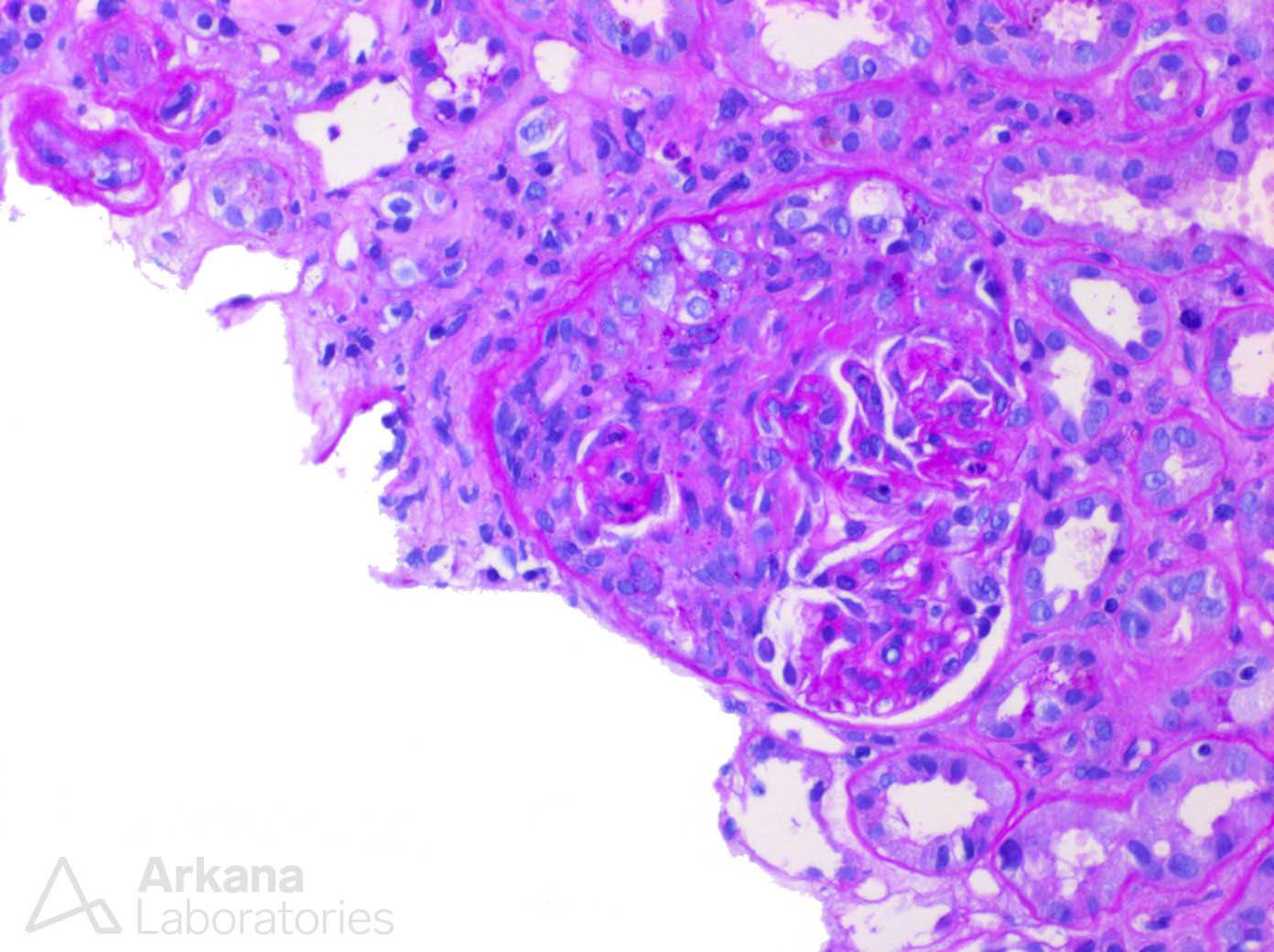
The image shows a glomerulus with a fibrocellular crescent dissecting portions of the glomerular tuft. Within the uninvolved portions of the glomerulus no obvious endocapillary proliferation is present and has the classic appearance of an ANCA-mediated glomerulonephritis. However, the immunofluorescence profile is unusual showing significant C3 deposition but pauci-immune heavy and light chains. Overall, these findings are most suggestive of endocarditis-associated glomerulonephritis. Endocarditis-associated glomerulonephritis displays a spectrum of light and immunofluorescence findings but can be troublesome as a mimic for ANCA-mediated glomerulonephritis and should be considered when atypical findings present in what appears by light microscopy to be ANCA-mediated glomerulonephritis. In Boils CL, Nasr SH et al study (see reference), most patients with endocarditis-associated glomerulonephritis showed reduced serum C3 levels, ≥2+ staining for at least 1 immune reactant, negative MPO and PR3 (significant minority are ANCA+ however), IV drug abuse/HCV positive, or a prosthetic valve. In our patient presented here, there was a history of prosthetic valve, reduced serum C3, and she was found to have endocarditis after kidney biopsy via trans-esophageal echocardiogram.
Reference: Boils CL, Nasr SH, et al. Update on endocarditis-associated glomerulonephritis. Kidney Int 2015 Jun;87(6):1241-9. https://www.ncbi.nlm.nih.gov/pubmed/25607109
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.