The patient is a 70-year-old white female who presents with 4 gm/24 hr proteinuria and a creatinine of 1.2 mg/dl. She has colon cancer with metastases to the liver, treated with chemotherapy and Avastin. The patient has recently had anemia, thrombocytopenia, ascites, and a urinary tract infection treated with nitrofurantoin. Her blood pressure has been under good control at 120/80.
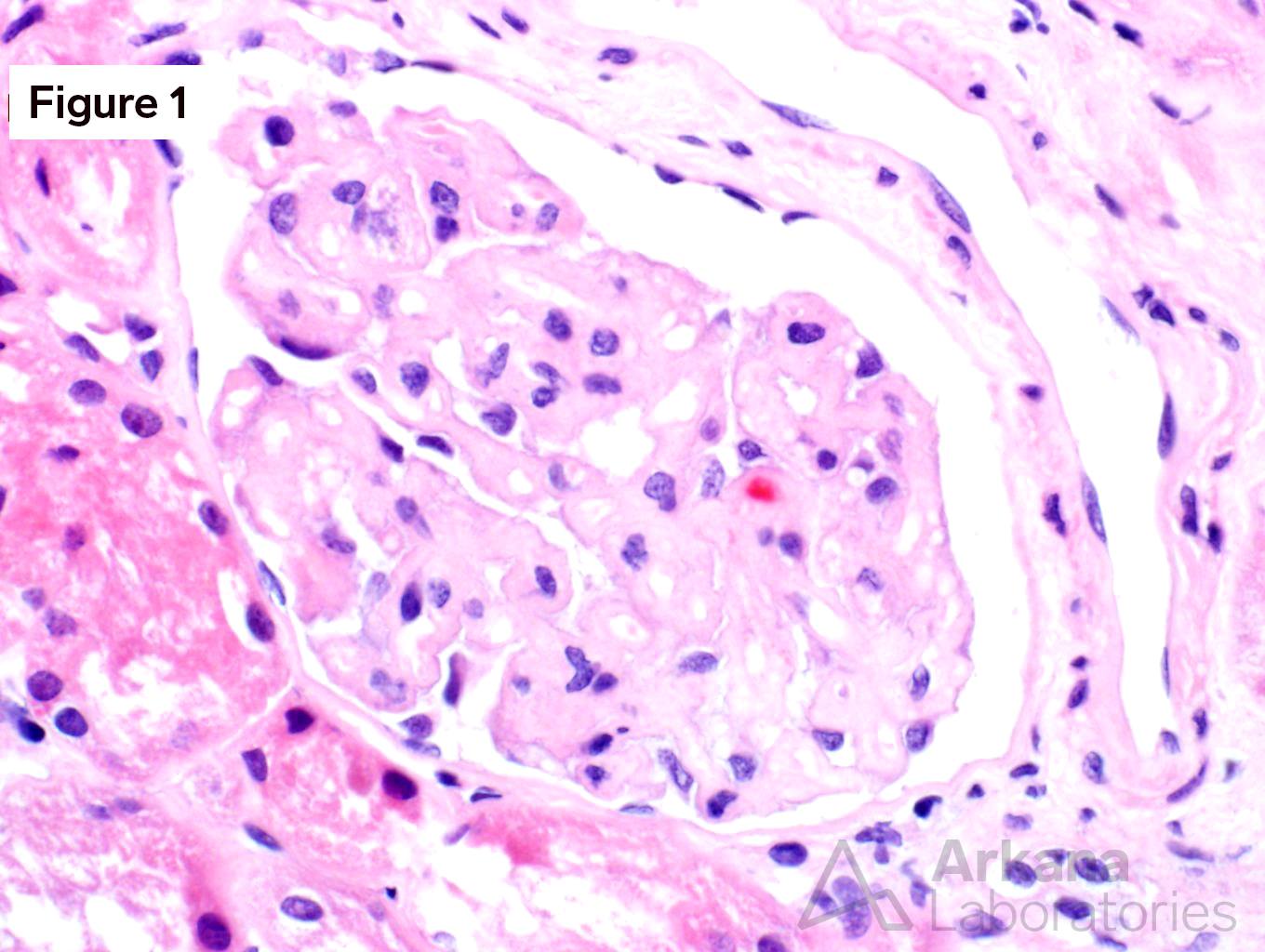
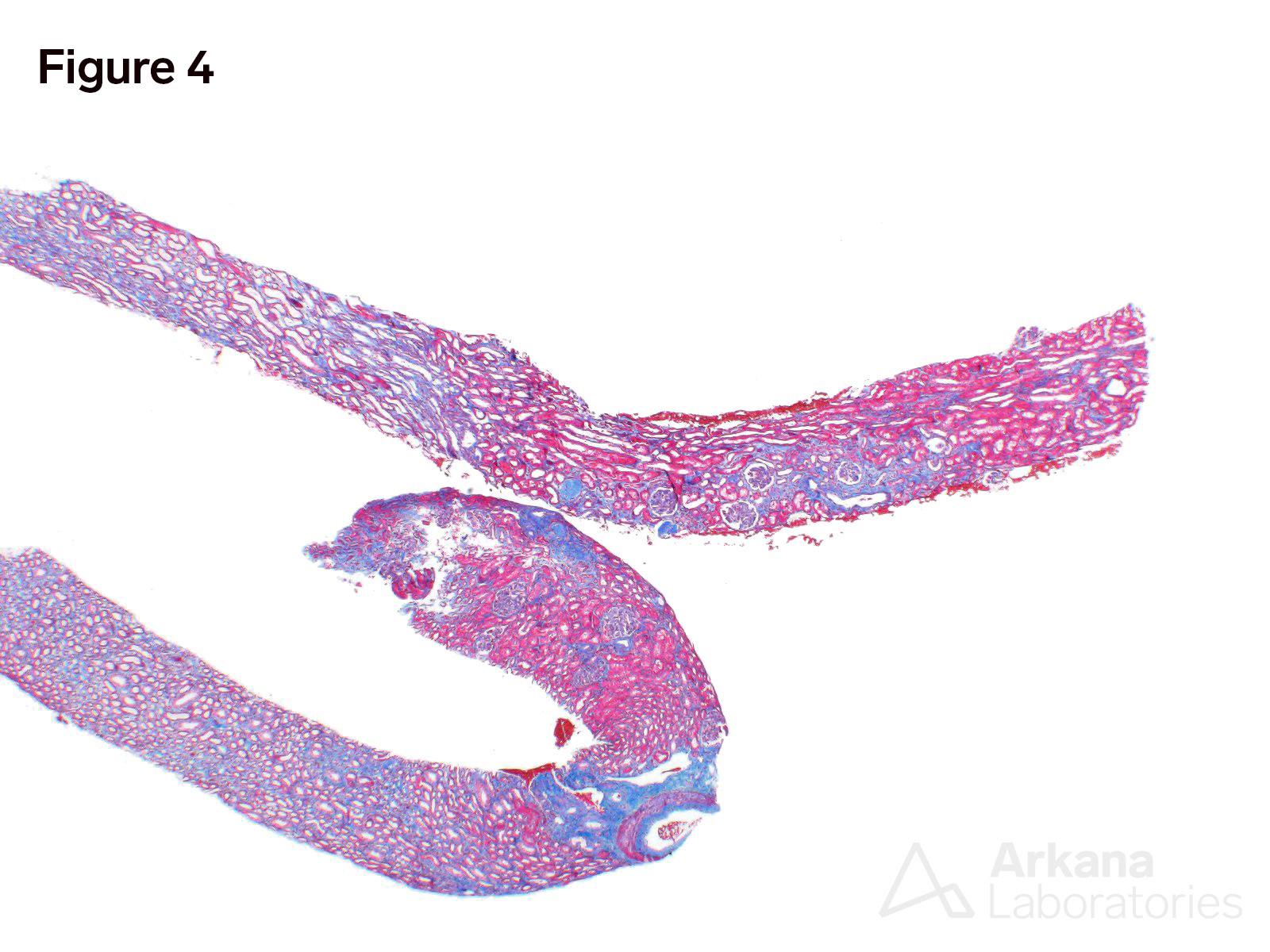
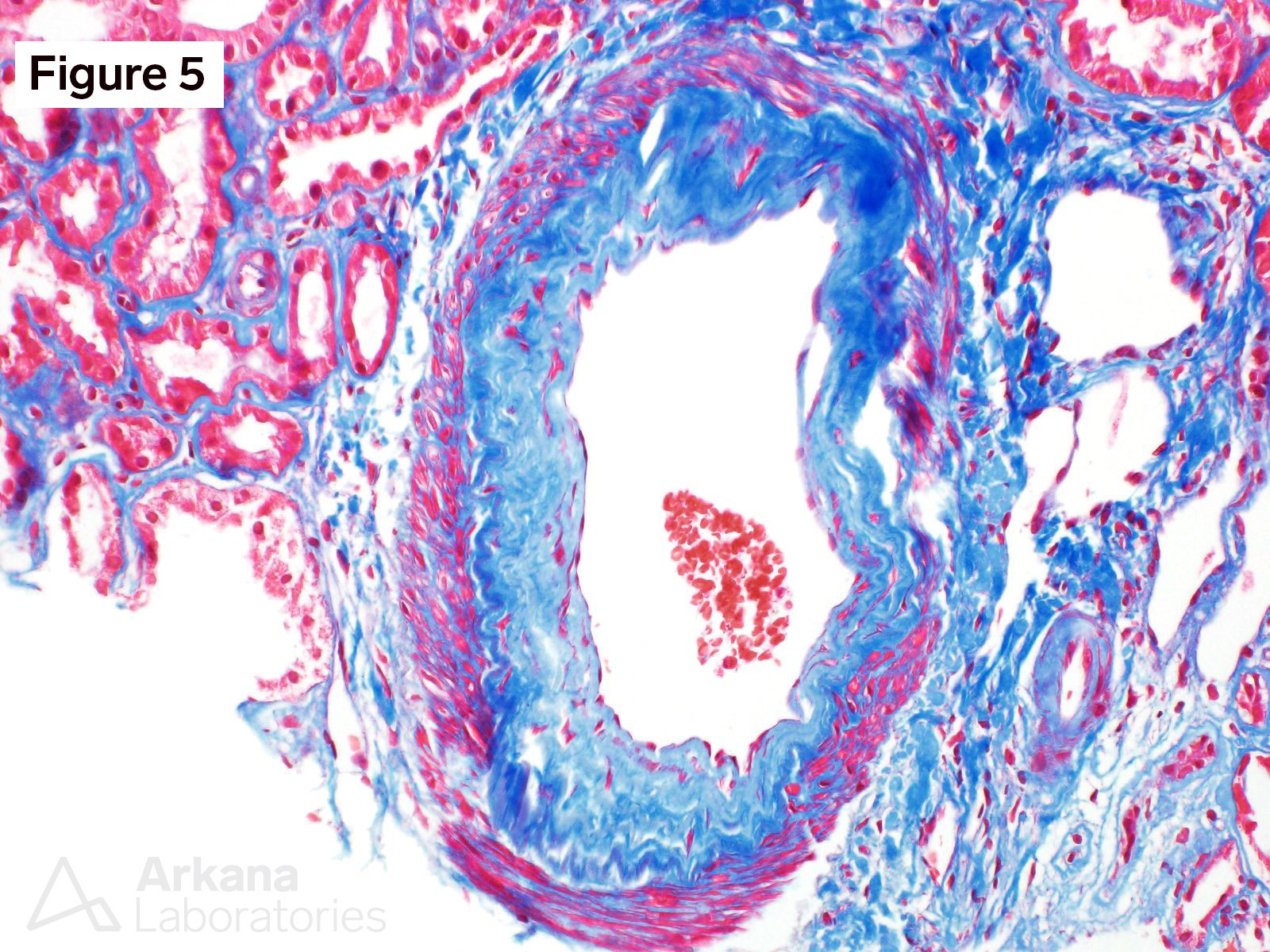
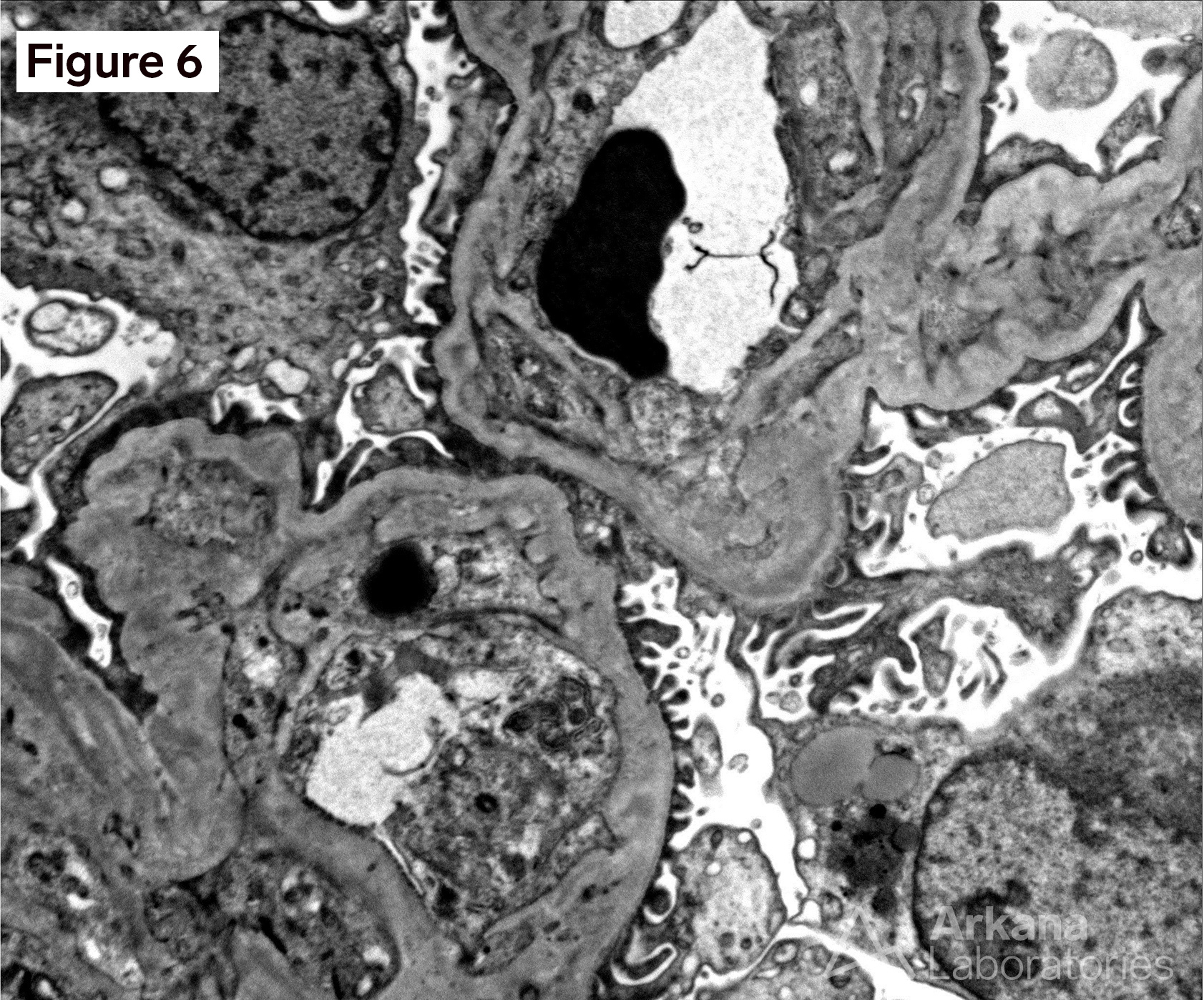
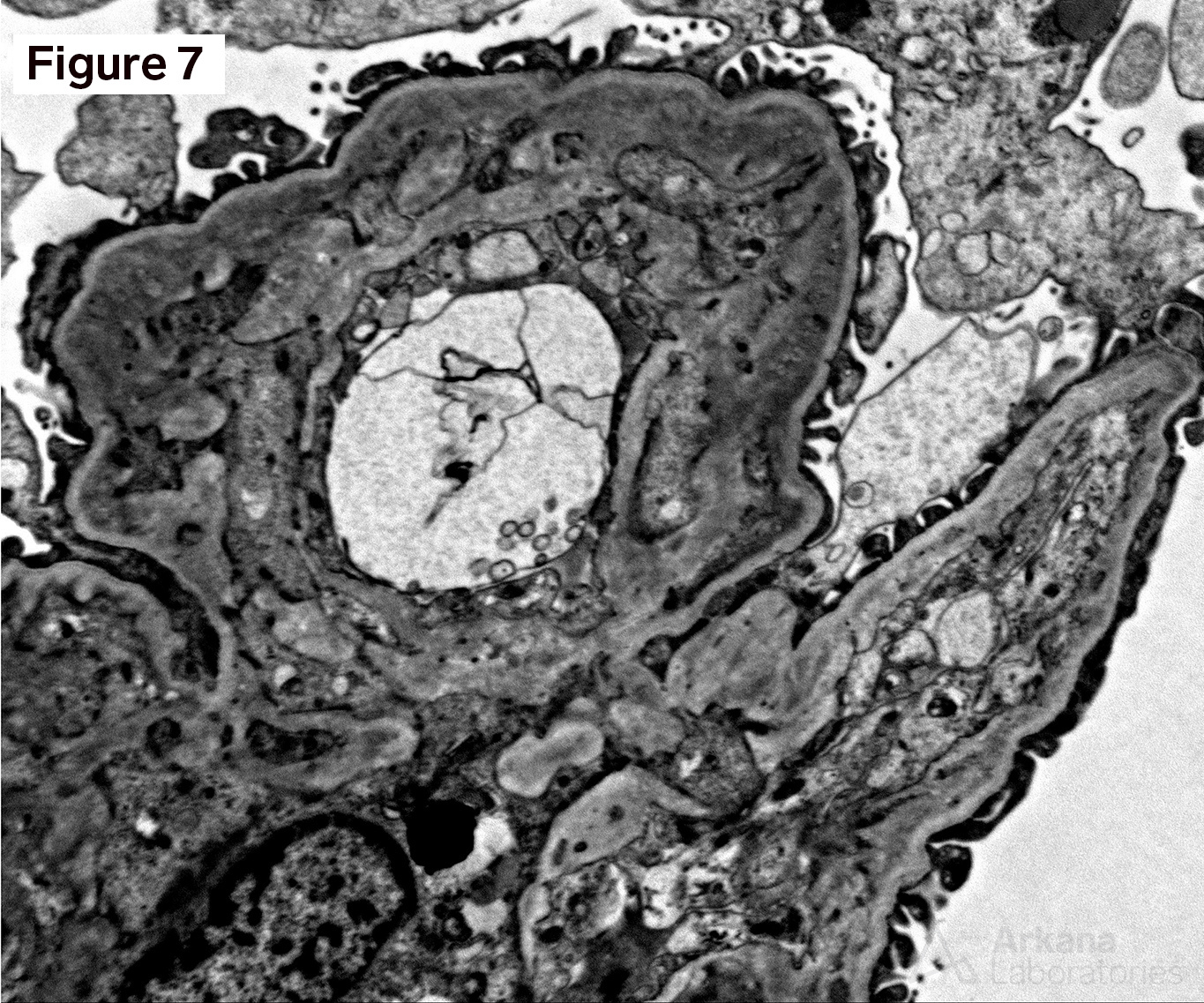
Figure 1 shows acellular closure of the capillary lumens and a “cotton-candy” appearance of the mesangium. Figures 2 and 3 shows capillary microaneurysms and segmental capillary hyalinosis. Figure 3 additionally shows double contours. Figure 4 shows moderate interstitial fibrosis. Figure 5 shows severe arteriosclerosis. Figure 6 and 7 shows subendothelial expansion and neo-basement membrane production with cellular interposition.
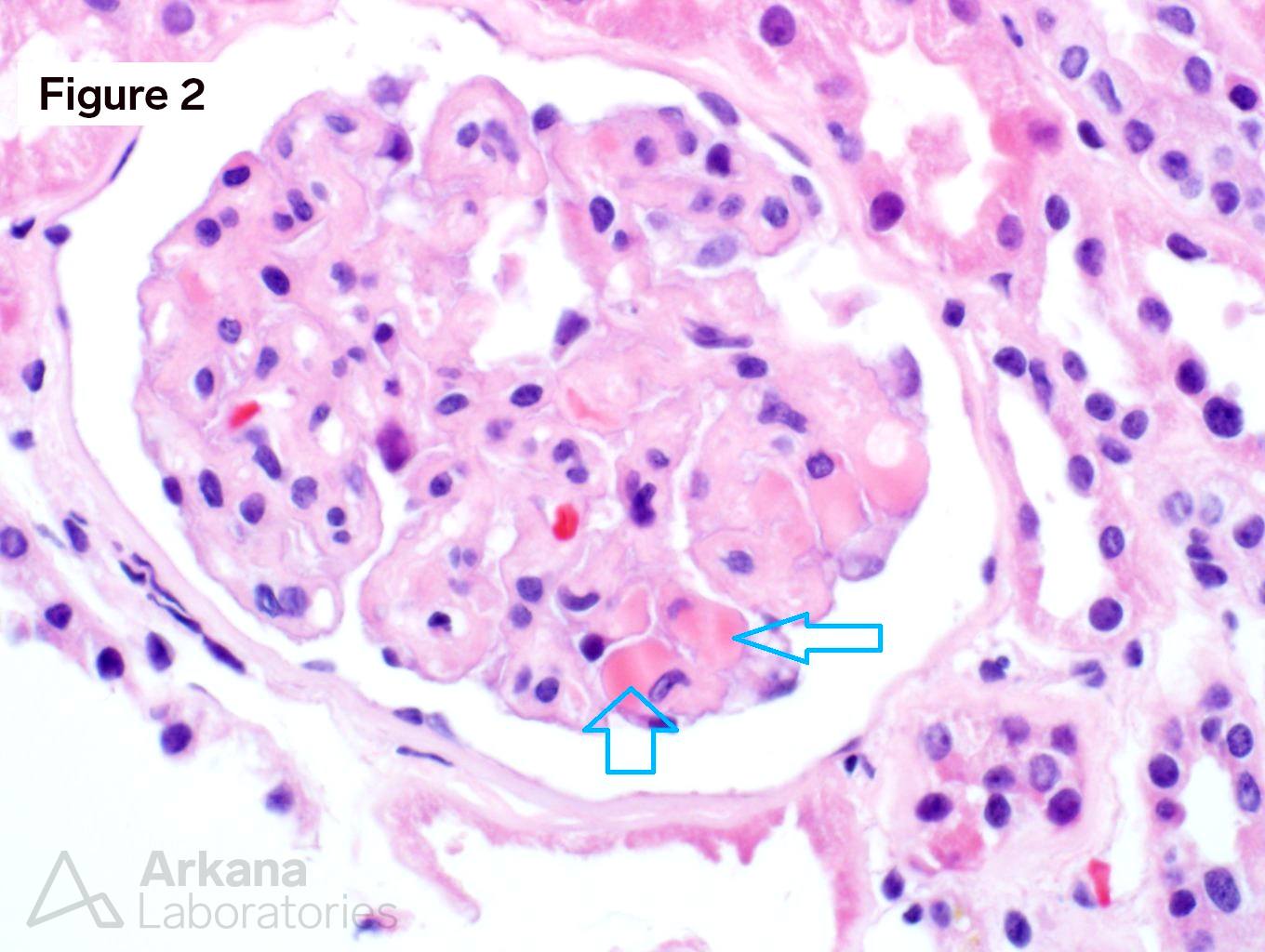
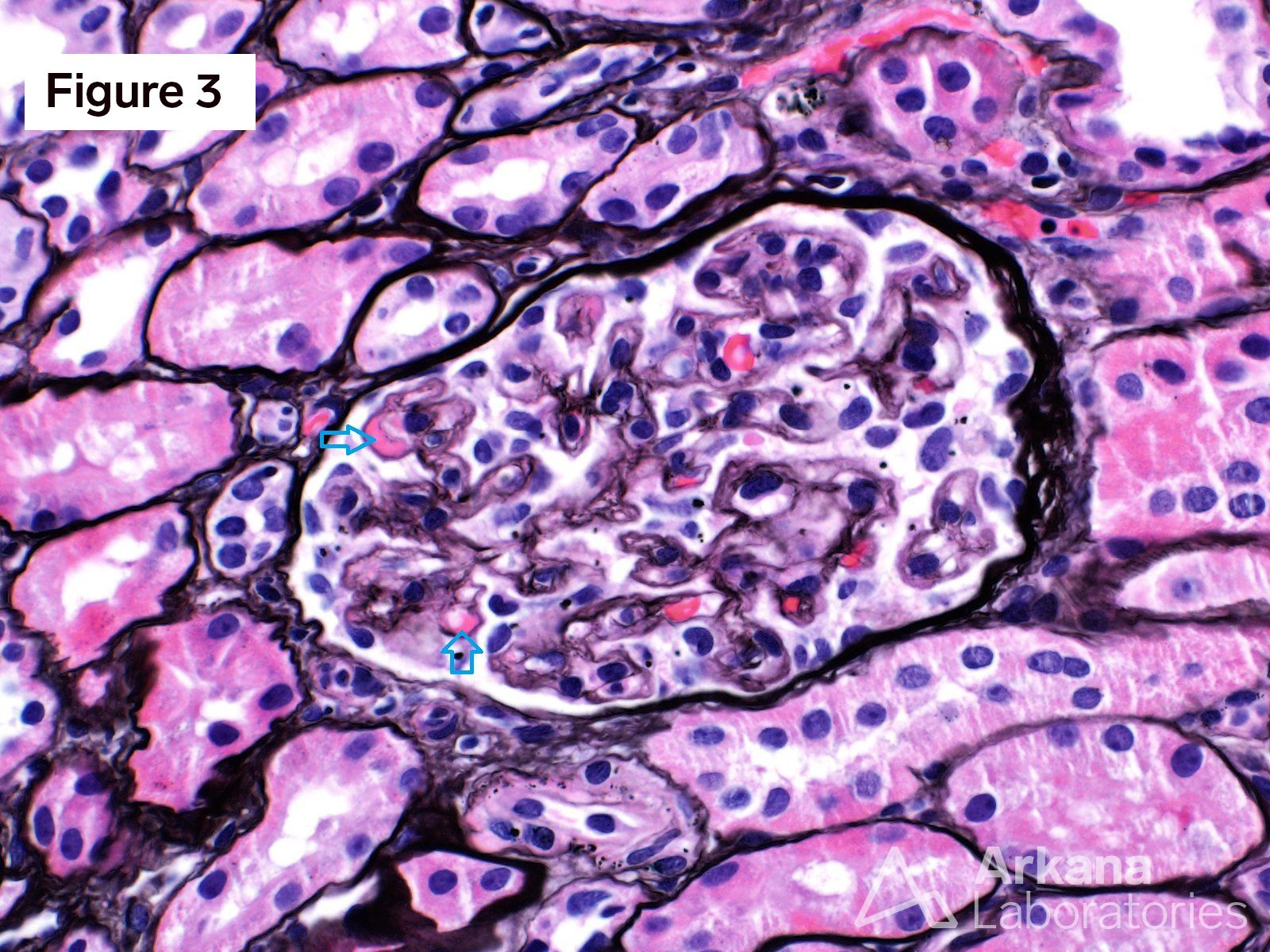
This is a case of anti-VEGF therapy-induced glomerular microangiopathy (aVEGF-GMA). The glomeruli have characteristic capillary microanerurysms and segmental capillary hyalinosis. “Double contours”, as seen here, are found in almost all cases however, the periglomerular vessels are usually unremarkable. Unlike some forms of thrombotic microangiopathy, all glomeruli are typically involved in aVEGF-GMA. And, glomerular fibrin thrombus formation is rare as are fragmented RBCs. Experiments within transgenic mice have shown a similar morphologic pattern of microaneurysms and segmental hyalinosis in mice challenged with anti-VEGF inhibitor. The differential diagnosis for anti-VEGF therapy-induced glomerular microangiopathy includes diabetic glomerulopathy, immune-complex type membranoproliferative pattern glomerulonephritis, and cryoglobulinemic glomerulonephritis. In diabetic glomerulopathy, mesangial expansion and Kimmelstiel-Wilson nodule formation is commonly found in addition to the segmental capillary hyalinosis. Immune-complex type membranoproliferative pattern glomerulonephritis and cryoglobulinemic glomerulonephritis have mesangial and endocapillary hypercellularity in addition to positive immunofluorescence staining. Immunofluorescence staining can be seen within aVEGF-GMA, but the immunofluorescence reactivity is usually observed only within the hyalinosis and not the true granular deposits seen in MPGN or cryoglobulinemia. Clinically, almost all patients with aVEGF-GMA present with nephrotic range proteinuria. And, when the anti-VEGF drug is stopped further damage to the kidney is typically precluded.
https://www.ncbi.nlm.nih.gov/pubmed/30014486
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.