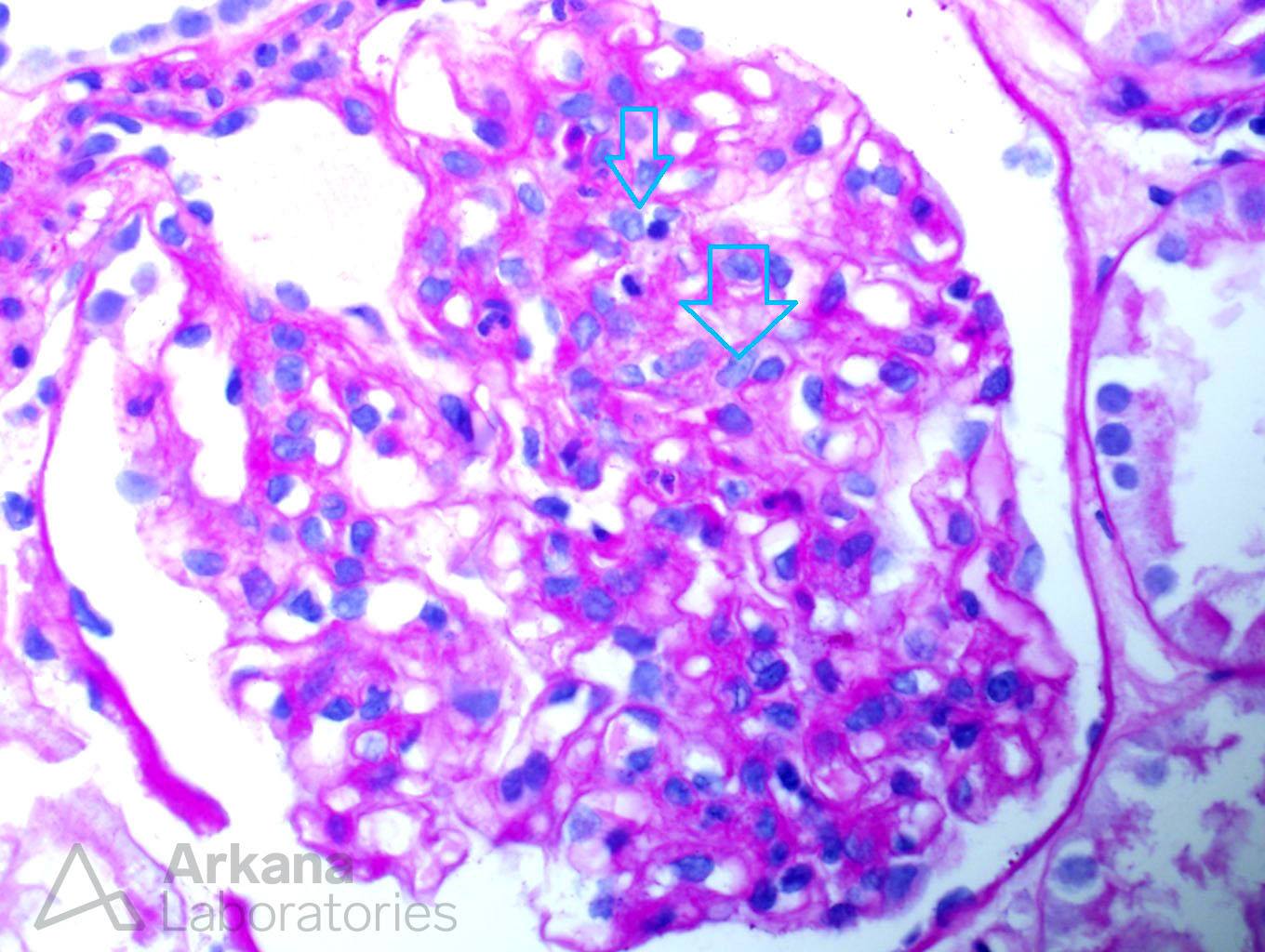
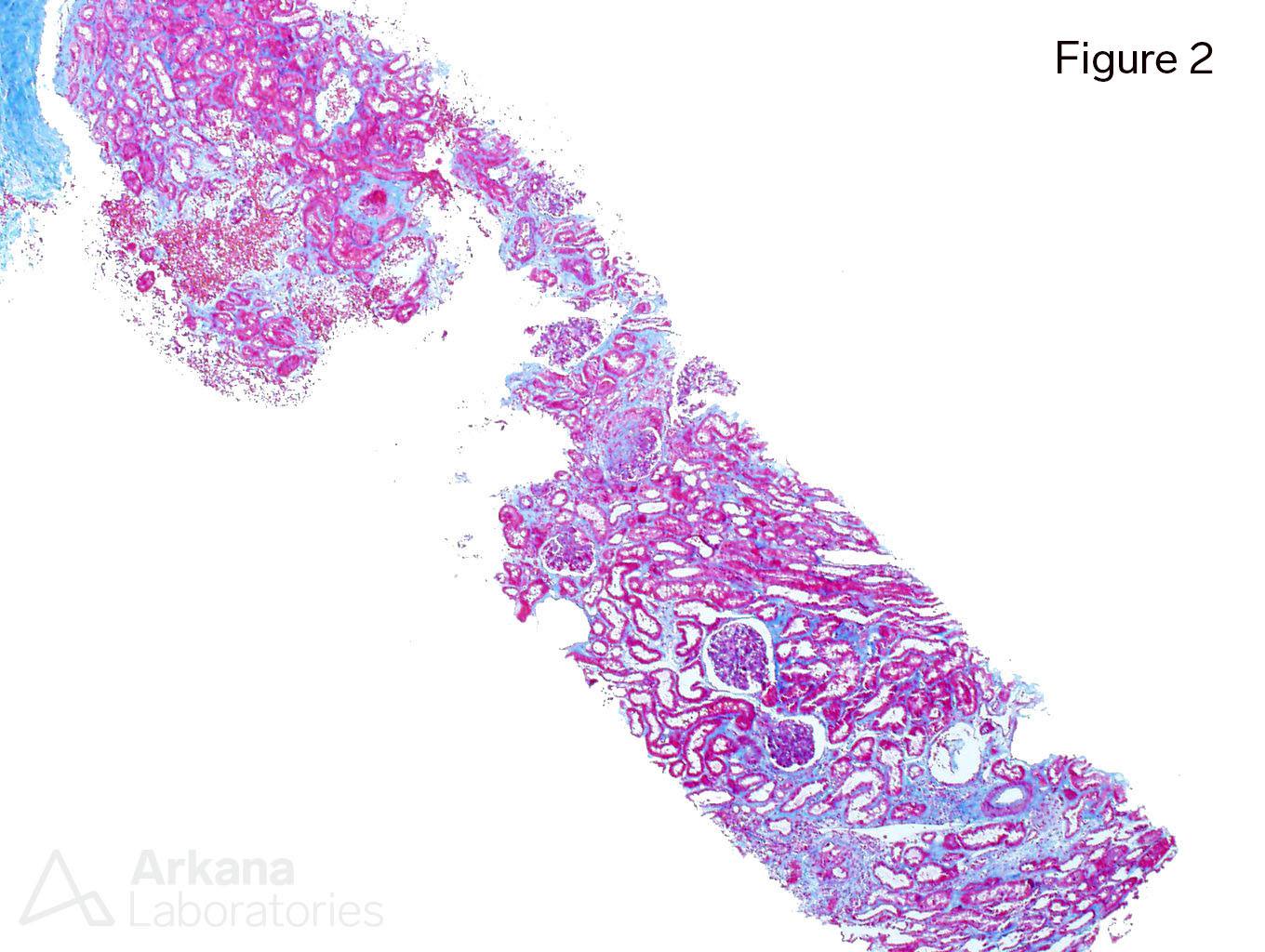
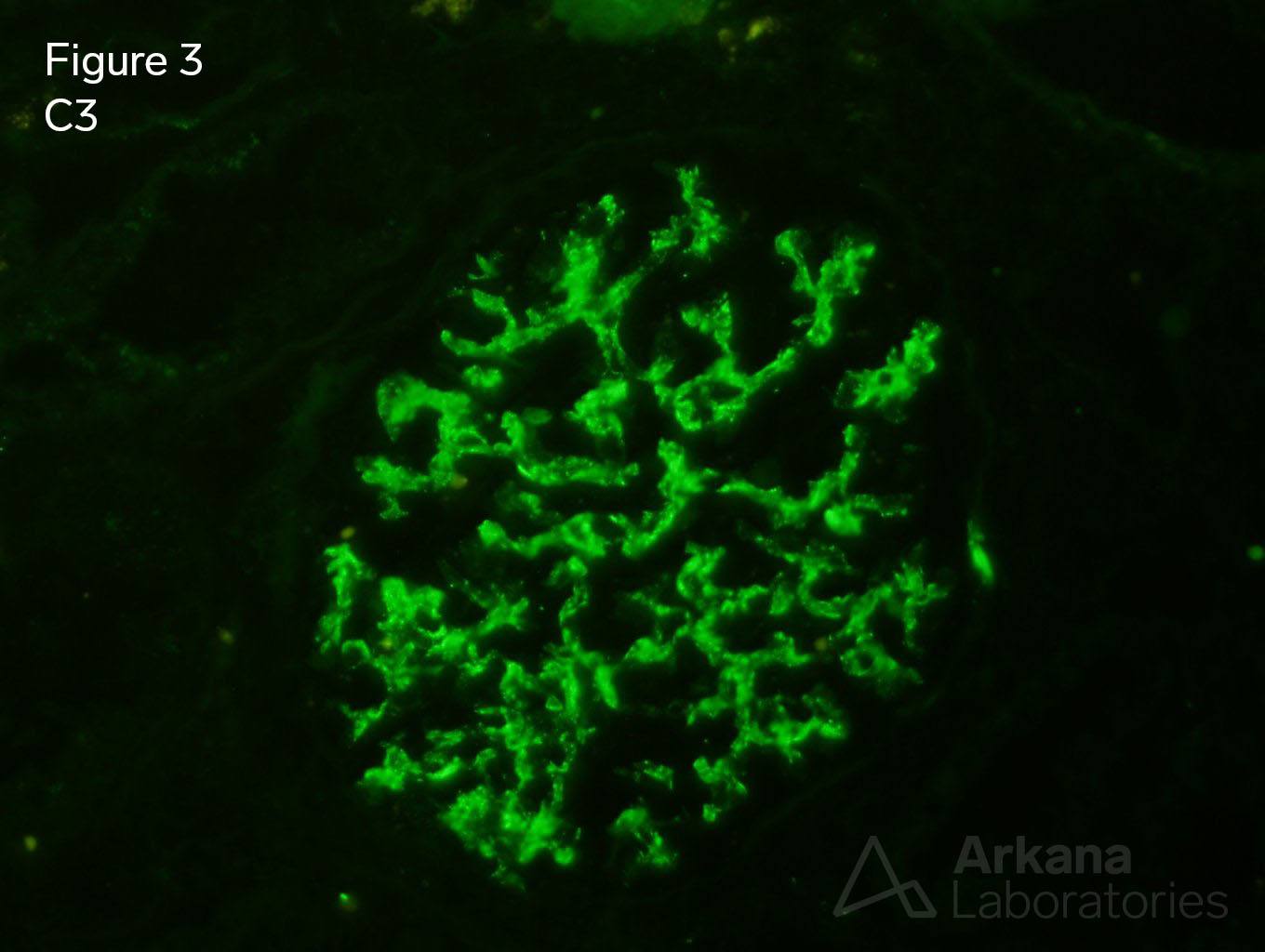
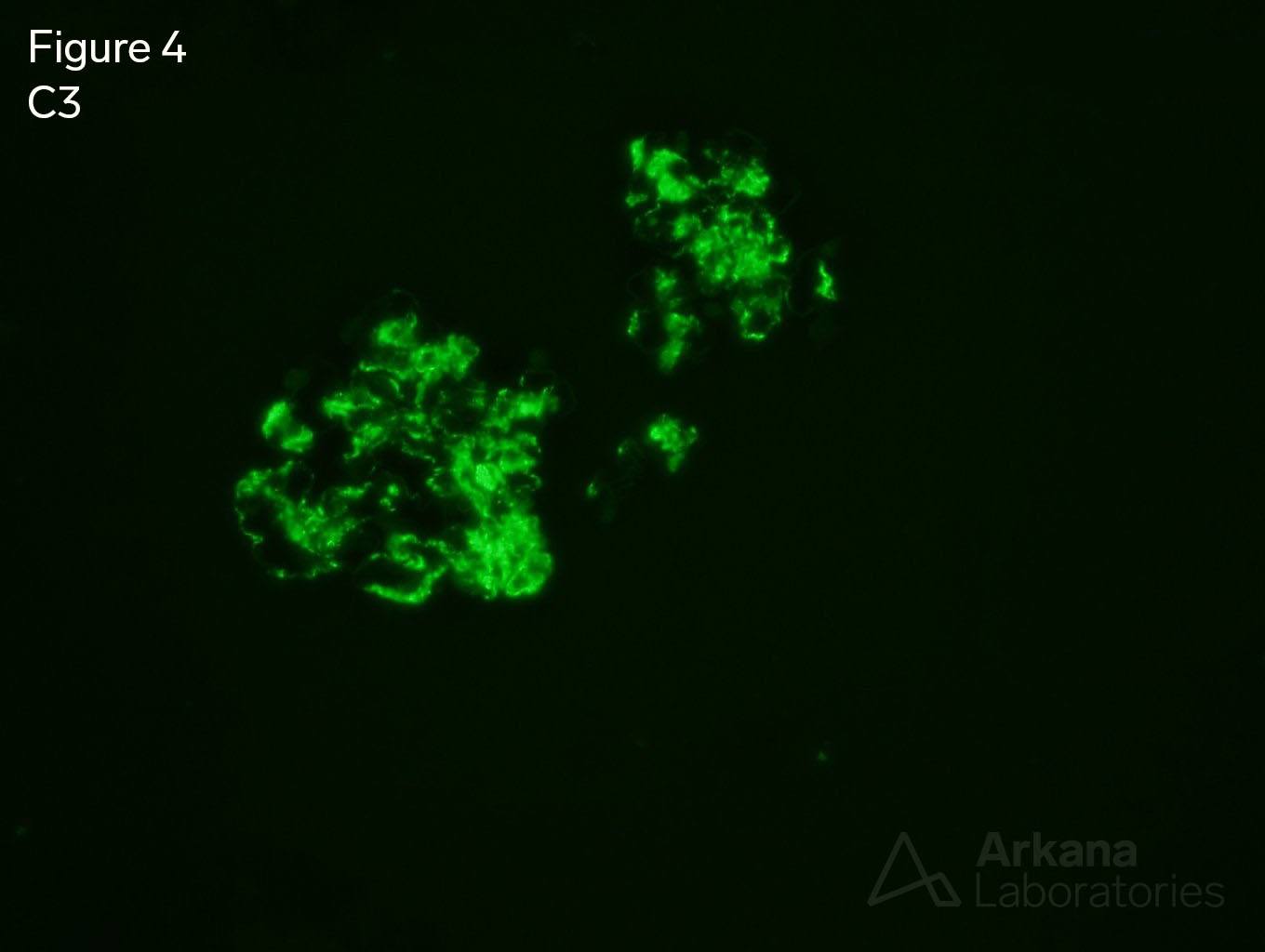
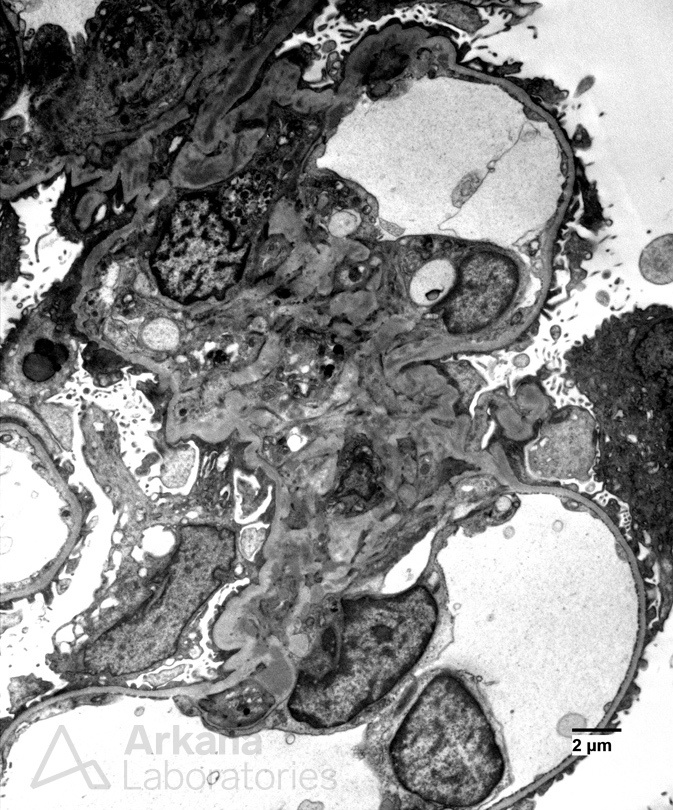
A 60-year-old male presents with a painful left hip, hematuria, and a creatinine of 1.5 mg/dl. He was recently hospitalized due to fever and chills. It was found that his left hip implant was infected. Blood cultures grew out methicillin-resistant Staphylococcus aureus. After beginning treatment with antibiotics and planning for surgery, a nephrology consult was requested. A kidney biopsy was performed and serologies were ordered. Figure 1 shows segmental endocapillary hypercellularity. Figure 2 shows mild interstitial fibrosis. Figure 3 shows staining with C3 only. All other immunofluorescence stains were negative on the frozen tissue. Immunofluorescence was then performed on the paraffin-embedded tissue to un-mask other immunoreactants. C3 was positive on the paraffin-embedded tissue (Figure 4). Figure 5 shows mesangial electron-dense deposits.
The kidney biopsy shows focally proliferative glomerulonephritis with C3 staining only. With the clinical history, the diagnosis of infection-associated glomerulonephritis is most likely, although C3 glomerulonephritis cannot be definitively excluded. If infection-associated, then treatment of the underlying infection should resolve this focal glomerulonephritis. However, should persistent, low serum C3 level and hematuria occur after treatment, then the possibility of C3 glomerulonephritis is more concerning and may warrant an investigation into dysregulation of the complement system.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.