Clinical History:
- CC: The patient is a 76-year-old woman progressive lower extremity then upper extremity anesthesia and dysesthesia, right then left foot drop, difficulty ambulating, decreased dexterity, and neck and back pain.
- PMH: bilateral Achilles tendinitis, bilateral lower extremity atherosclerosis with claudication, chronic venous insufficiency, CCP antibody positive arthralgia, low back pain with sciatica, left ulnar nerve impingement, and peripheral arterial occlusive disease. Family history: cardiovascular disease.
- Medications: atorvastatin, gabapentin and meloxicam.
- Physical exam: no fasciculations; strength 5/5 bilateral upper extremities, 0/5 bilateral lower extremities in a wheelchair; reflexes: 1+ throughout except gastrosoleus 0, Hoffman normal, toes down going; sensation: reduced at ankle, normalizes above knee; extensive edema bilateral calves; gait: cannot test.
- MRI spine: significant neural foraminal stenosis of C-spine.
- Lab results: CSF normal.
- EMG: severe length dependent axonal peripheral neuropathy; chronic L5 and S1 radiculopathy. Clinical concern for neuropathy with or without vasculitis.
Based on history and images, what is the process of greatest concern?
A. Acute inflammatory demyelinating polyneuropathy
B. Giant cell arteritis
C. Chronic inflammatory demyelinating polyneuropathy
D. Vasculitis
Answer:
Vasculitic Neuropathy
Asymmetric or patchy, neurogenic symptoms, especially with a stepwise progression suggest a vascular etiology, although both central and peripheral demyelinating disorders can show a similar progression. Foot drop, however, is especially worrisome specifically for vasculitis.
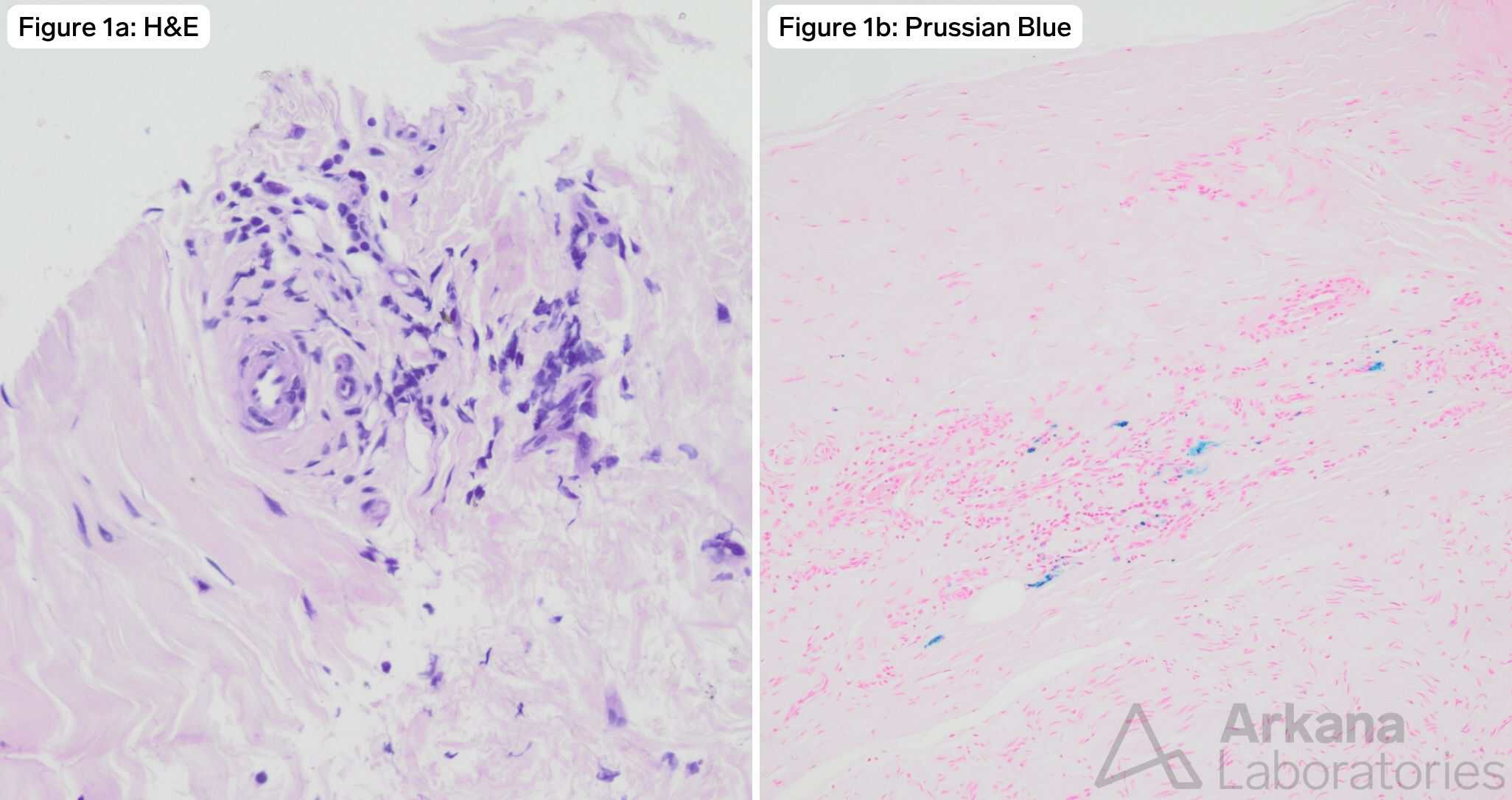
In this case, the H&E-stained sections show perivascular lymphocytic inflammation. This can be a nonspecific findings but is compatible with vasculitis. Prussian blue is a histochemical stain that reveals iron deposition as blue, suggesting prior microscopic bleeds. When found around small vessels in nerve biopsy, this is suspicious for vasculitis.
Vasculitis is one of the few, truly urgent diagnoses in muscle and nerve pathology. This is often a rapidly progressive disorder where delay of therapy can allow progression of irreversible injury to nerve and other organs. Although the diagnostic features of vascular wall injury and/or fibrinoid necrosis is not seen in this case, the possibility of vasculitis should be reported to the patient’s clinical team as soon as possible.
Serology plays a key role in diagnosing vasculitis. Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis is a systemic disorder that commonly involves the peripheral nervous system and presents as mononeuritis multiplex. Three systemic disorders are described: microscopic polyangiitis (MPA), granulomatosis with polyangiitis (GPA, aka Wegener granulomatosis), and eosinophilic granulomatosis with polyangiitis (EGPA, aka Churg-Strauss syndrome).[4] pANCA and MPO are most often associated with microscopic polyangiitis. cANCA and PR3 positivity is most often associated with Granulomatosis with polyangiitis (GPA; aka Wegener granulomatosis).
Reference(s) / Additional Reading:
- Chkheidze R, Pytel, P. JNEN. 2020;79(4):355–364.
- Collins MP, Hadden RD. Nat Rev Neurol. 2017;13(5):302-316.
- Collins MP, Kissel JT, et al. J Peripher Nerv Syst. 2010;15(3):176-84.
- Koike H. 2022;11(1):21-38.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.