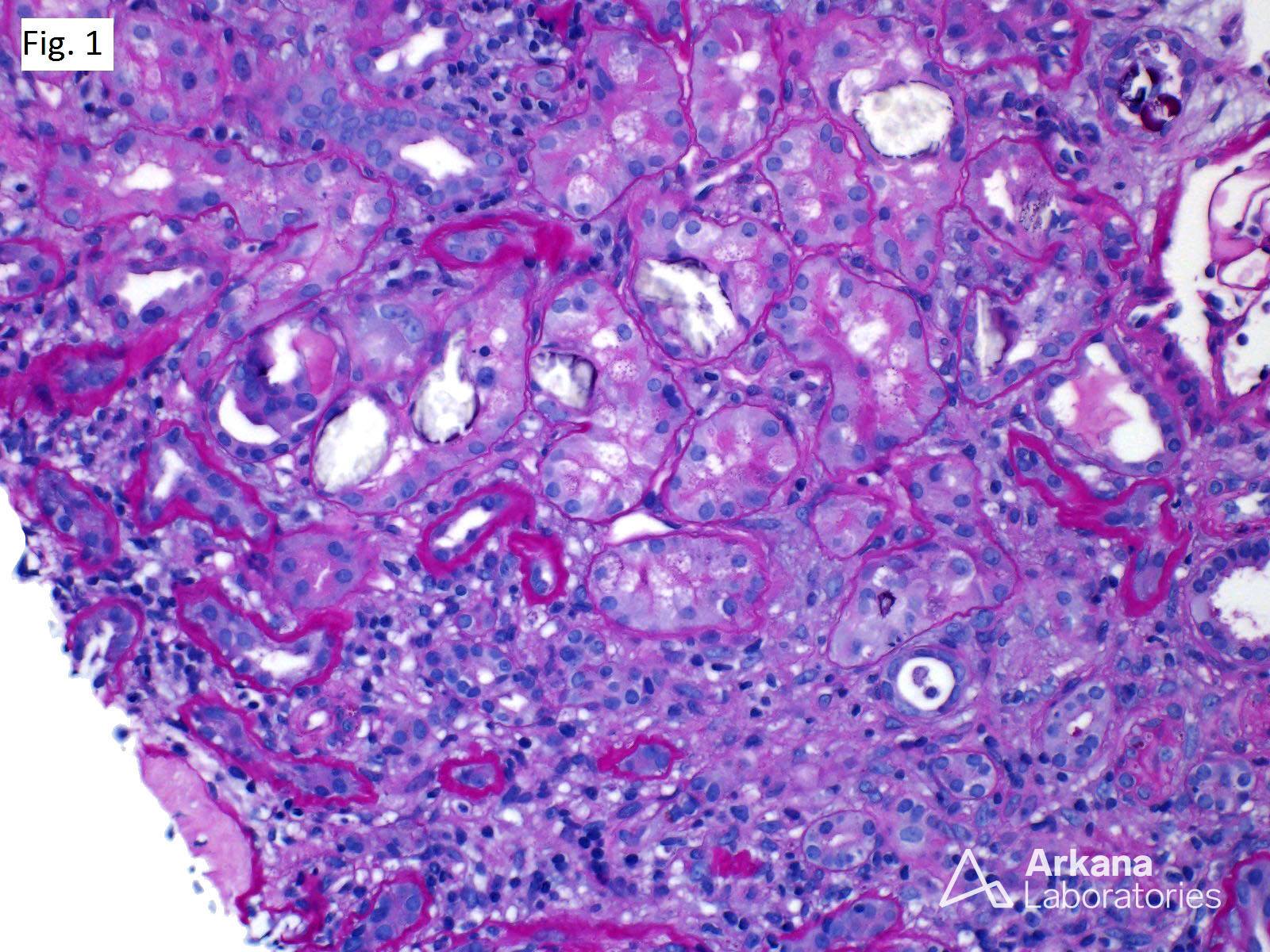
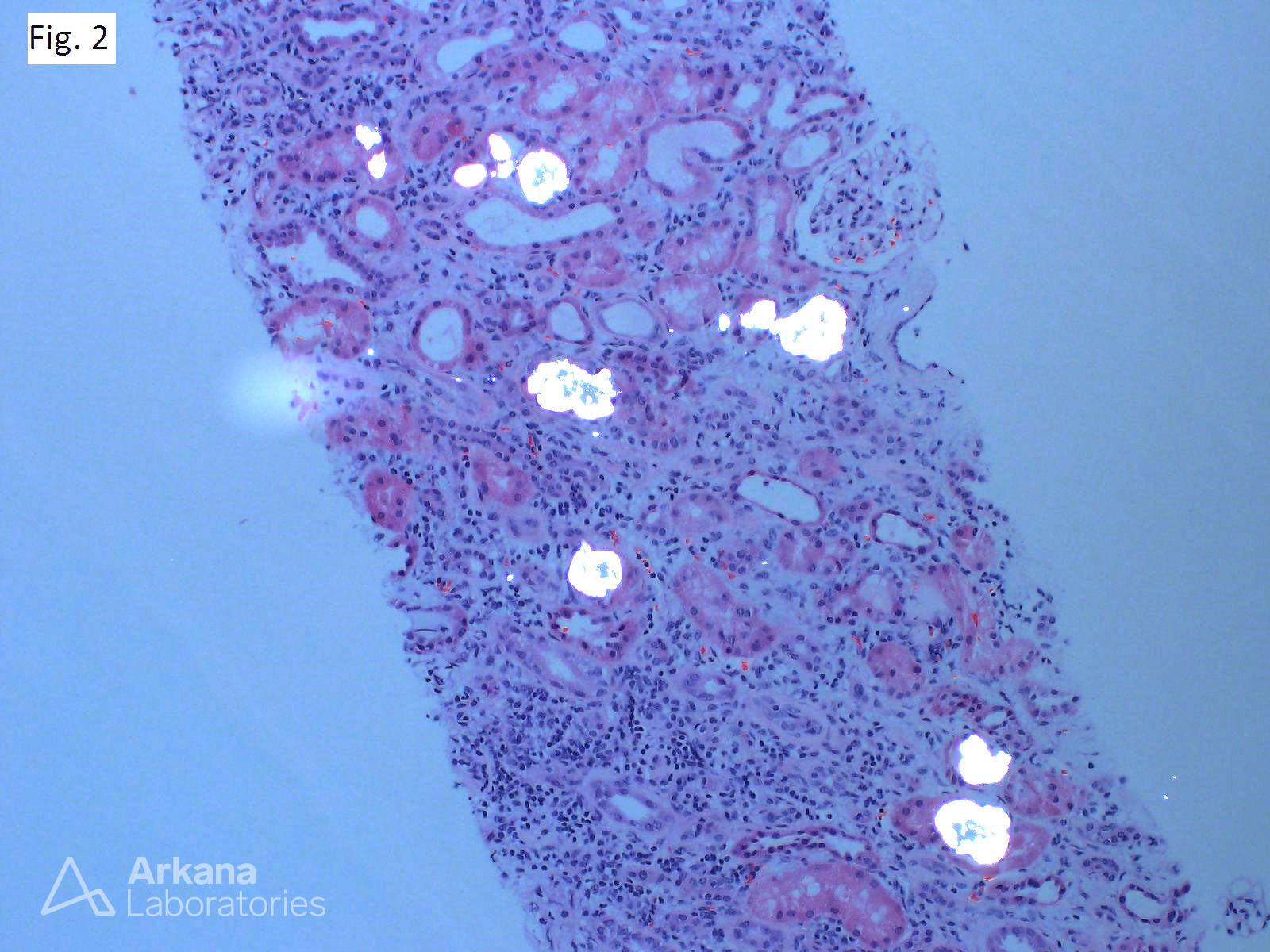
H&E stained section (Fig. 1) demonstrating acute tubular injury with frequent translucent intratubular crystalline deposits on a background of severe tubulointerstitial scarring. The crystals show birefringence under polarized light (Fig. 2) characteristic of renal oxalosis. After the biopsy, this 60-year-old male admitted consumption of small quantities of ethylene glycol over the past 16 months. Other causes of secondary renal oxalosis include enteric forms (Crohn’s disease, celiac sprue, pancreatic insufficiency, small intestinal or gastric bypass or resection), over-ingestion of oxalate containing foods (e.g., dark leafy vegetables, rhubarb, kale, starfruit, tea, spinach, sesame seeds, almonds, peanuts, beets, buckwheat flour, chocolate soy milk), absence of enteric oxalate-degrading bacteria (i.e., Oxalobacter formigenes), vitamin B6 deficiency, excess ascorbic acid ingestion, aspergillosis, drugs (Orlistat, Praxilene), and prolonged tubular injury.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.