A 62-year-old Asian male with a past medical history significant for ESRD secondary to hypertension S/P renal transplant (9 months ago) presents with a creatinine of 1.9 (baseline 1.2). The patient has had no previous episodes of rejection. The donor-specific antibody is negative. CMV, adenovirus and BK serology is pending.
What is the best diagnosis?
A. Acute Cellular Rejection, Banff Type 1B
B. BK Nephritis
C. Adenovirus
D. Acute Antibody-Mediated Rejection
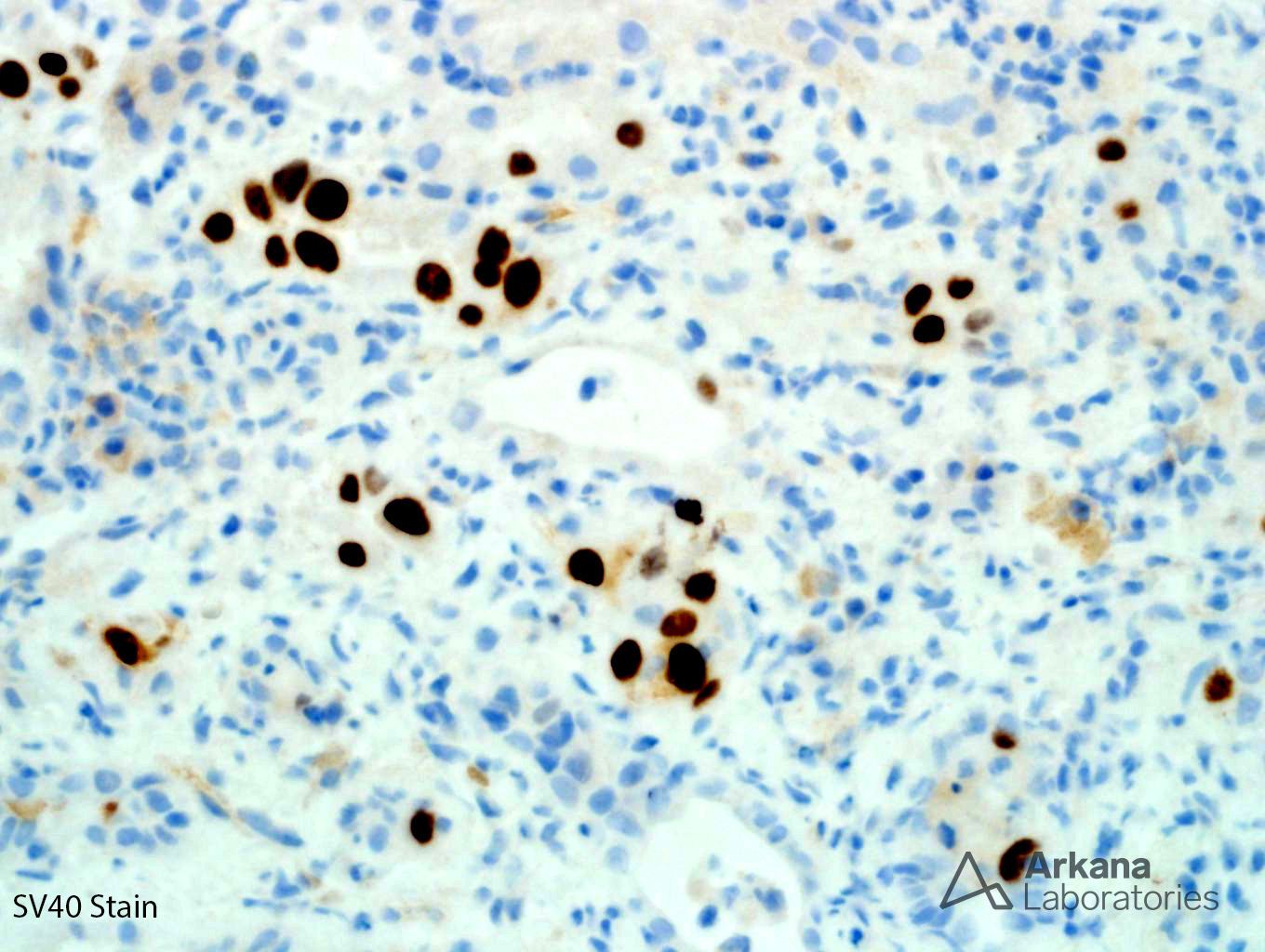
The correct answer is B (BK nephritis).
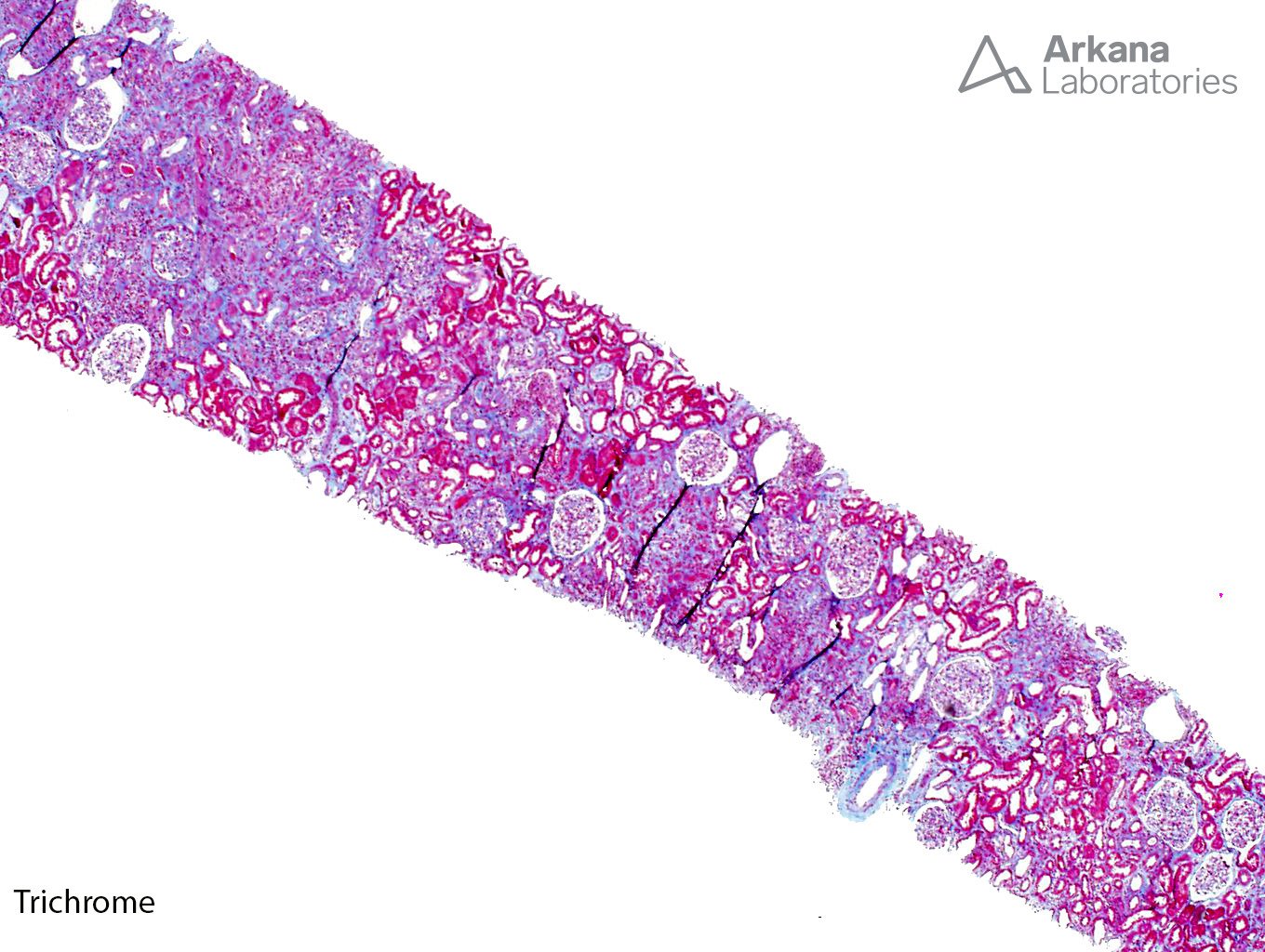
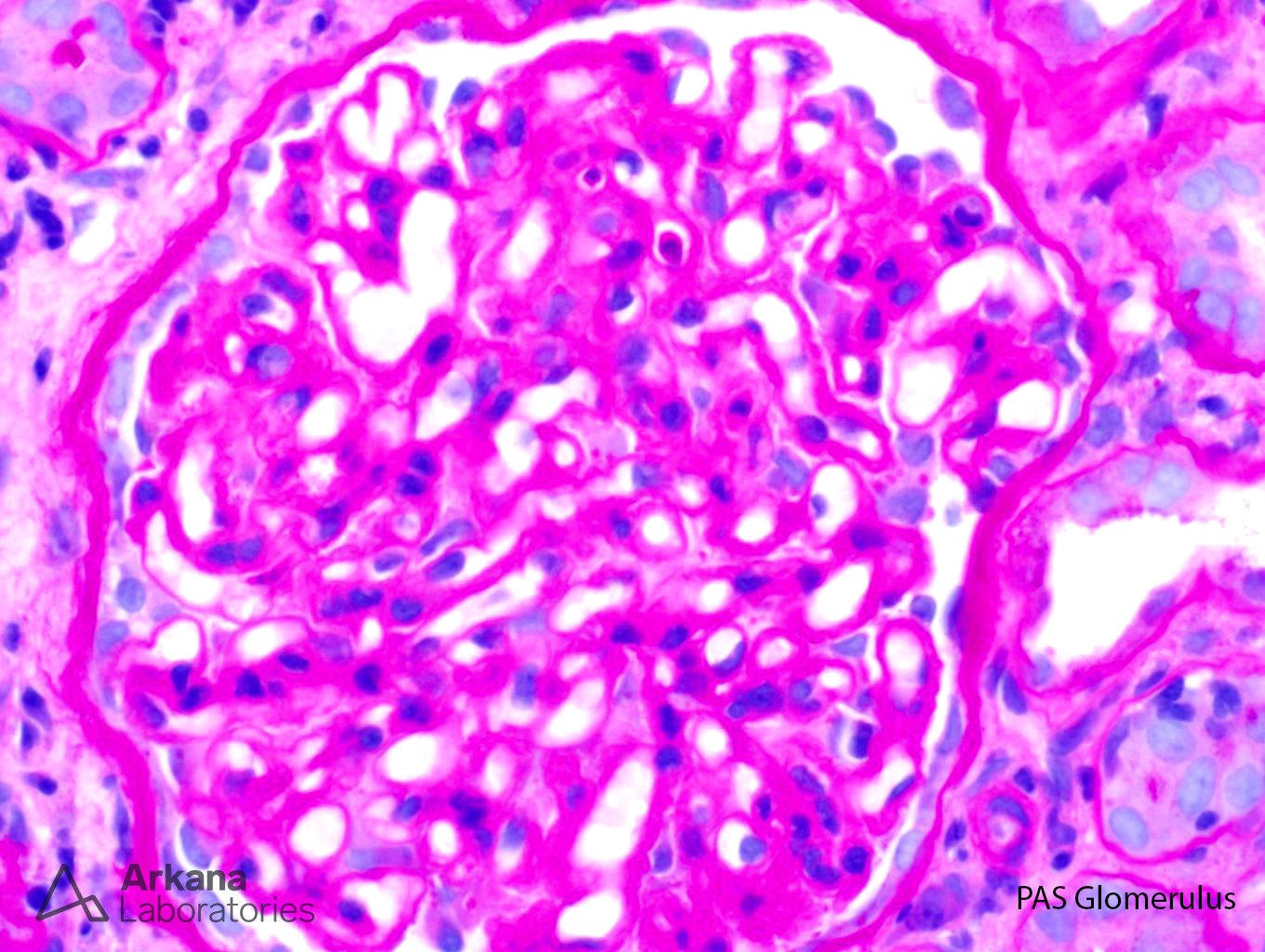
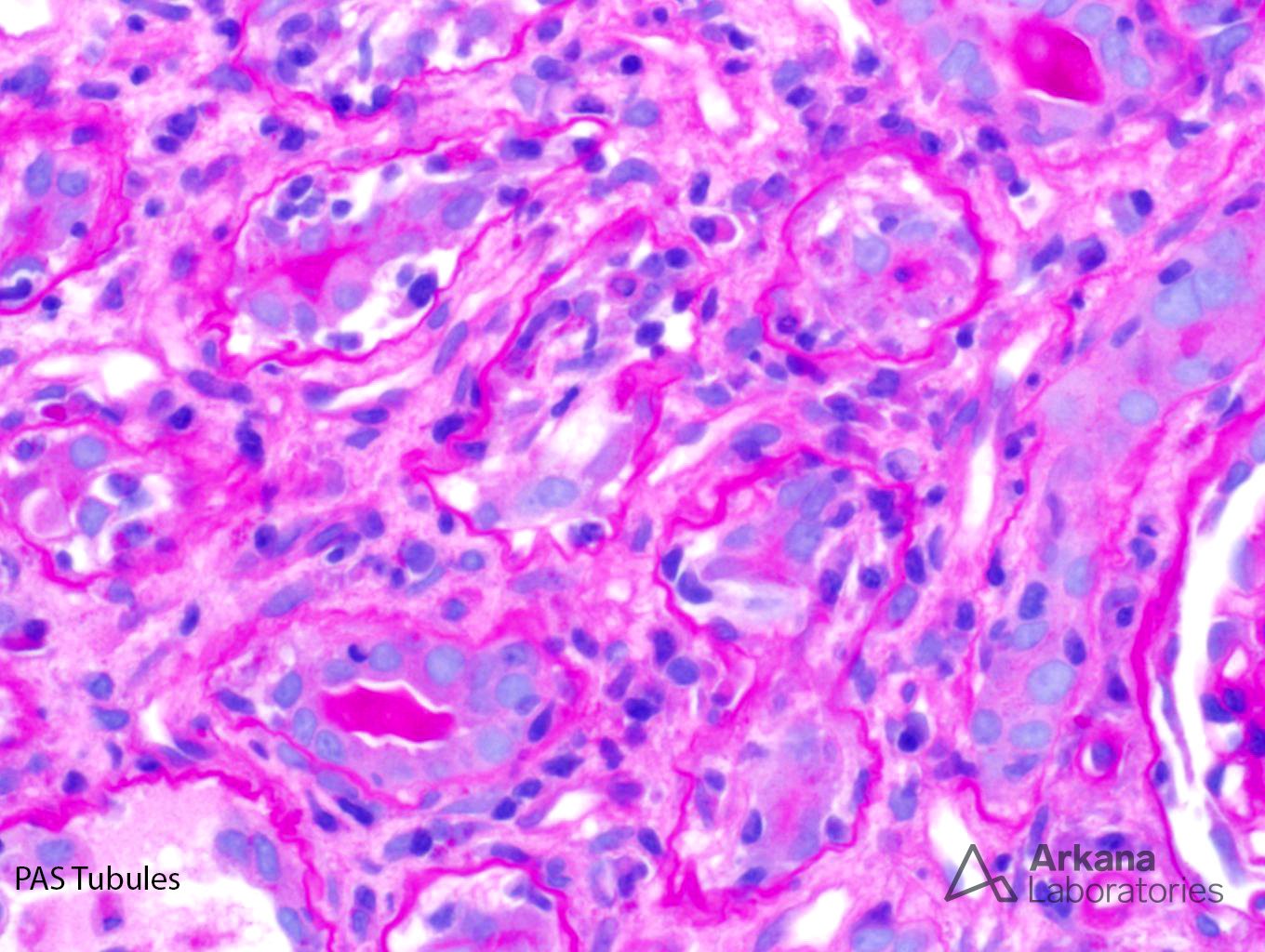
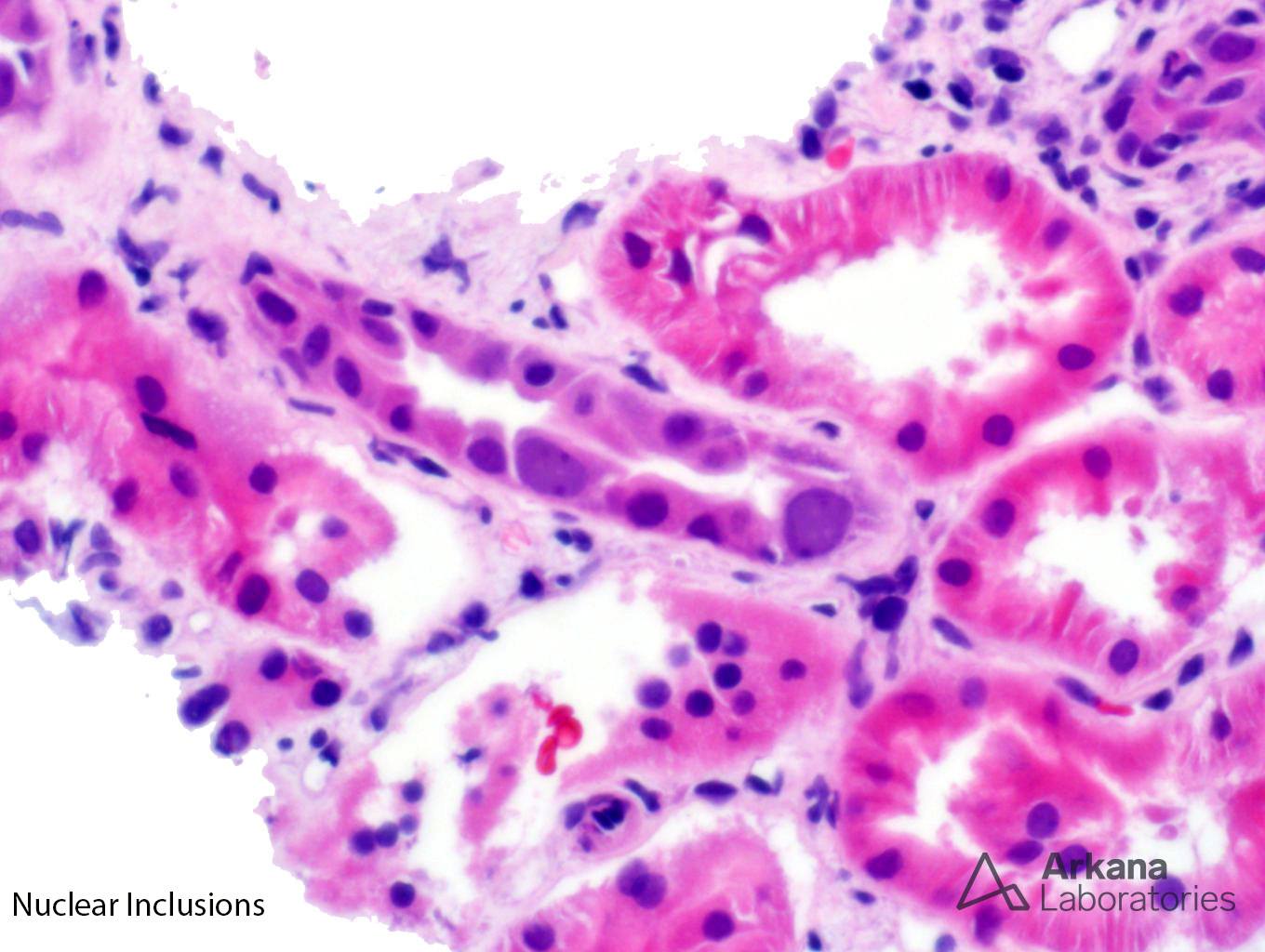
The low power trichrome picture shows patchy interstitial inflammation and fibrosis. The glomerulus has thickened capillary walls, but no definitive double contours are identified. The PAS stain shows marked tubulitis and a closer image of the PAS stain shows ground-glass nuclear inclusions. A SV40 stain confirms the presence of BK nephritis. Even though the biopsy does meet criteria for acute cellular rejection, the presence of positive SV40 inclusions precludes this diagnosis. Adenovirus has a different histological appearance consisting of numerous neutrophils and palisading necrosis. There is no evidence of glomerulitis and peritubular capillary margination to support a diagnosis of acute antibody mediated rejection.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.