Clinical History:
- History: 68-year-old man with 1 week of bilateral proximal upper and lower extremity weakness and 1 month of facial, eyebrow, neck, chest, and back rash (initially diagnosed as seborrheic dermatitis)
- PMH: HTN, PVD, asthma, hyperlipidemia, GERD, type 1 DM with retinopathy, IgA deficiency, hypothyroidism, former light smoker
- FH: Stroke, diabetes, arthritis, cancer, macular degeneration, heart disease
- Meds: Atorvastatin, insulin, levothyroxine, zolpidem; treated with Solu-Medrol and prednisone
- Physical exam: Mild-moderate proximal weakness, lower extremity edema
- MRI: Diffuse heterogeneous edema of bilateral quadriceps, adductors, and sartorius, suspicious for inflammatory myopathy
- Labs: CK peaked at 1570, trending down to 680; aldolase 20; mildly elevated CRP; ANA, Lyme, and RF negative; HMGCR Ab, MG panel, extended myositis and ENA panels pending
The primary pathology shown here is:
A. Necrotizing myopathic process
B. Eosinophil mediated inflammatory process
C. T-cell mediated inflammatory process
D. Macrophagic myofasciitis
Answer:
A. Necrotizing myopathic process
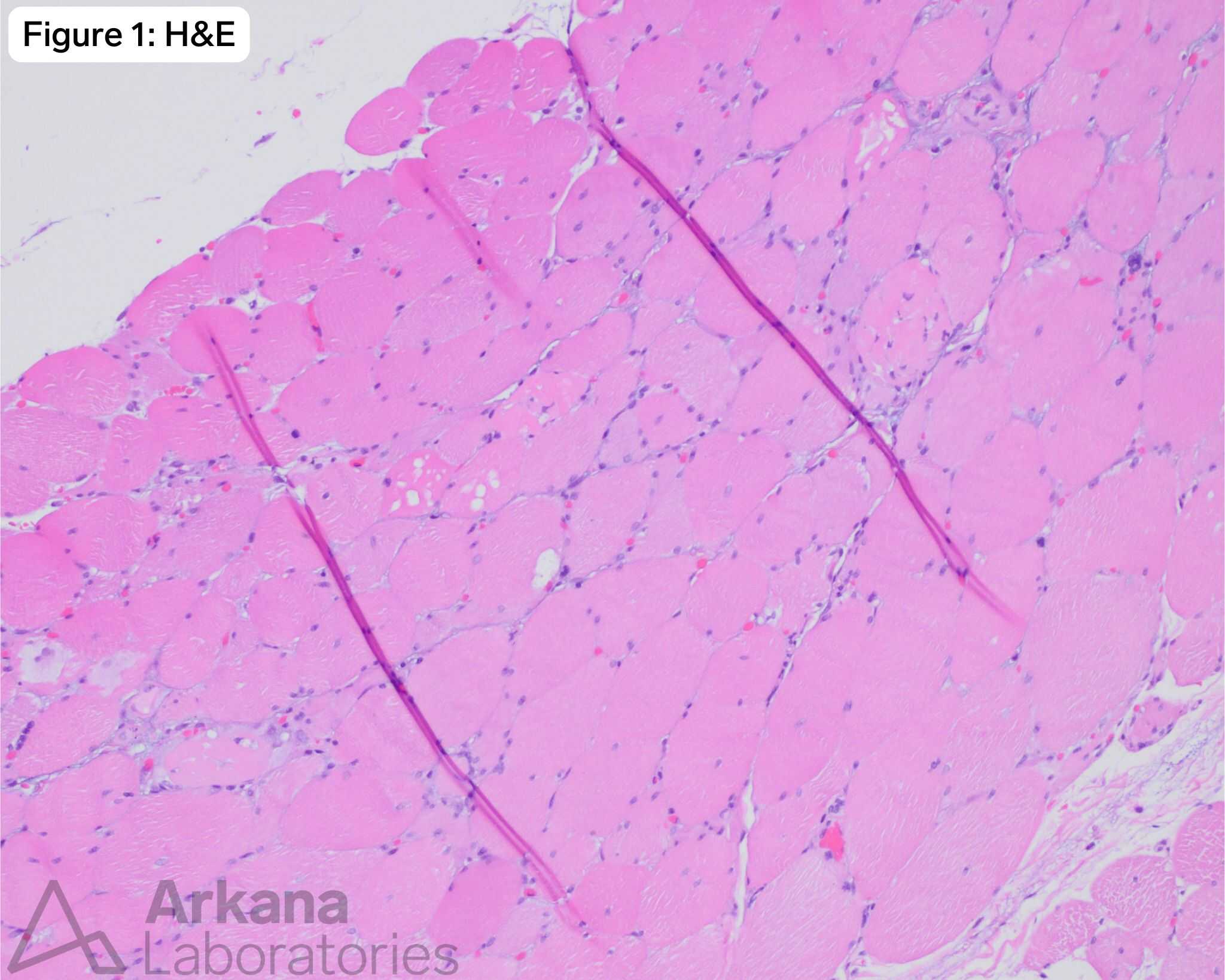
Pathology of necrotizing myopathy seen in this case:
- Basophilic (regenerating) fibers and mildly vacuolated hypereosinophilic (necrotic) fibers.
- No significant inflammatory cell infiltrate.
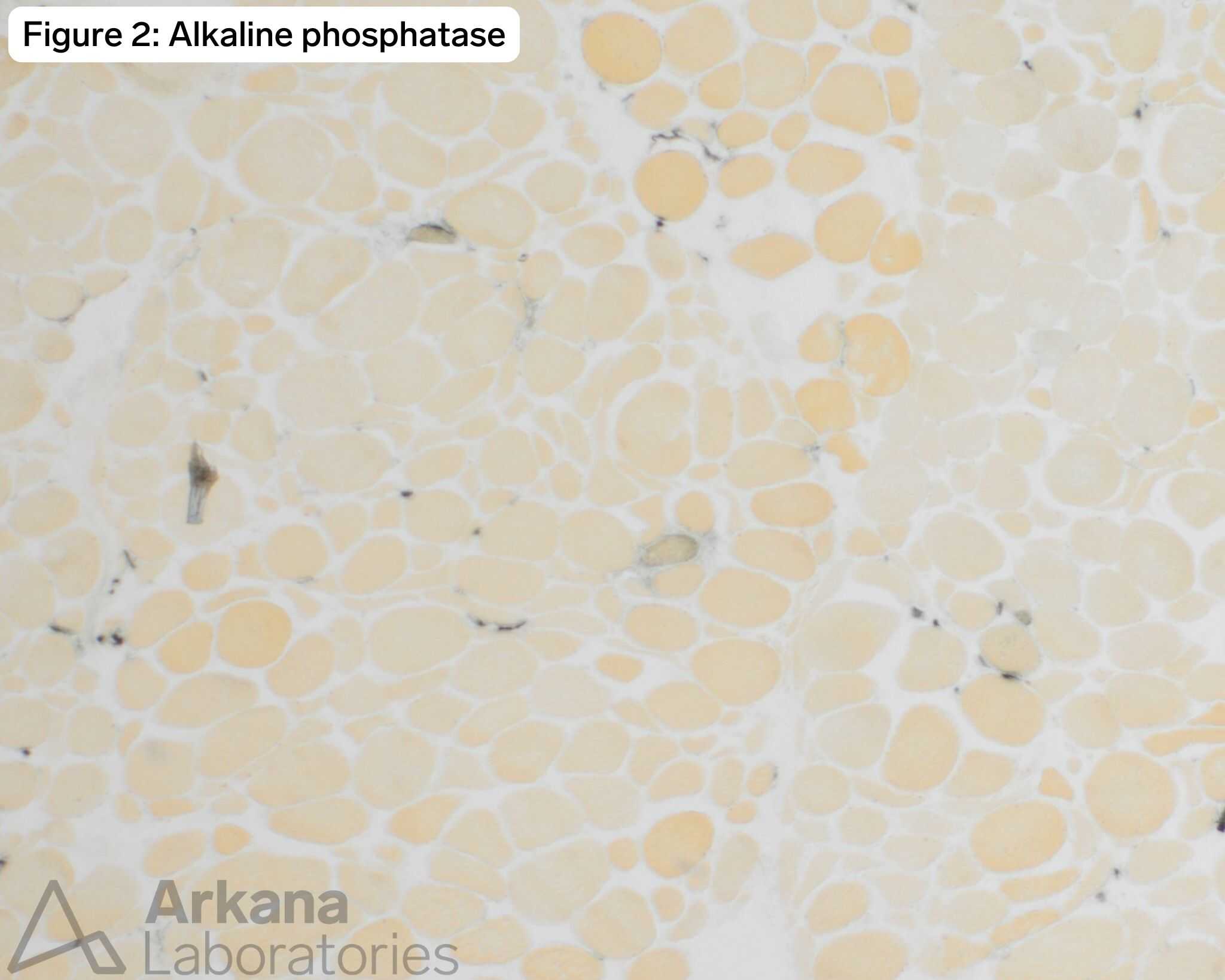
- Alkaline phosphatase dark regenerating fibers.
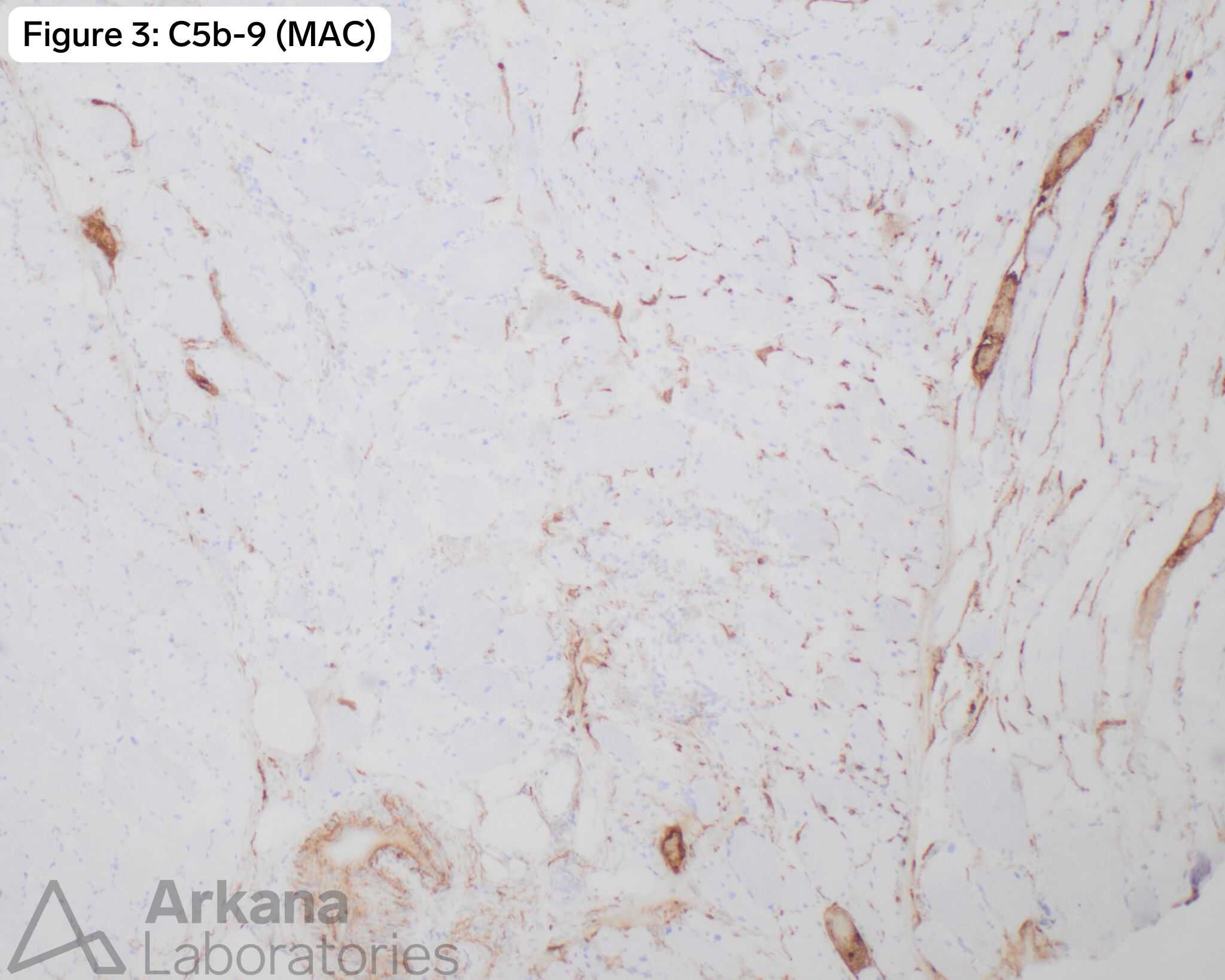
- Compliment C5b-9 (Membrane Attack Complex) positive necrotic fibers.
This is a setup for necrotizing myopathy. Common etiologies:
- Toxic myopathy (e.g. statin therapy)
- Immune-mediated necrotizing myopathy (IMNM; often with positive SRP or HMGCR serology)
- Partially treated idiopathic (acquired) inflammatory myopathy (myositis)
- Other etiologies include antisynthetase syndrome, and paraneoplastic, metabolic, endocrine (thyroid), or infectious (viral) myopathies.
However this month, all of the cases have the same history! It’s one patient with 4 concurrent, likely related diagnoses:
- Vasculitis of small muscular artery
- Myopathic changes
- Chronic active neurogenic changes
- MxA reactivity with perimysial pathology
Reference(s) / Additional Reading:
- Conticini E. Inflammatory muscle involvement in systemic vasculitis. Autoimmun Rev. 2022;21(3):103029.
- Waisayarat J. Sarcoplasmic Myxovirus Resistance Protein A. J Inflamm Res. 2023;16:5417-5426.
- Xing C. Myxovirus resistance protein A (MxA) expression in myositides. Muscle Nerve. 2024;69(5):548-555.
- Biopsy Diagnosis of Peripheral Neuropathy, 2nd Edition. JM Bilbao and RE Schmidt, eds. Springer, New York. 1995, 484 pp.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.