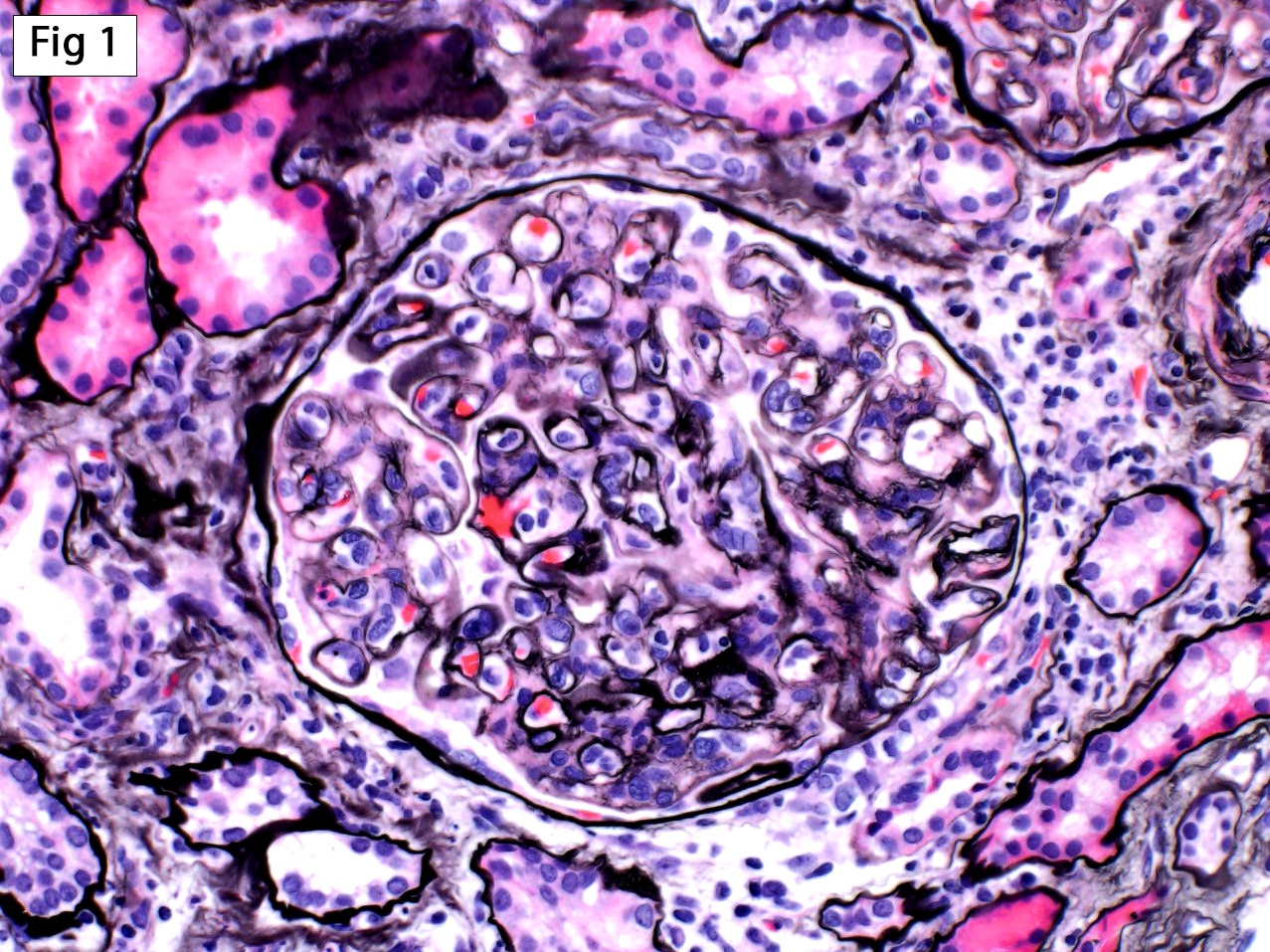
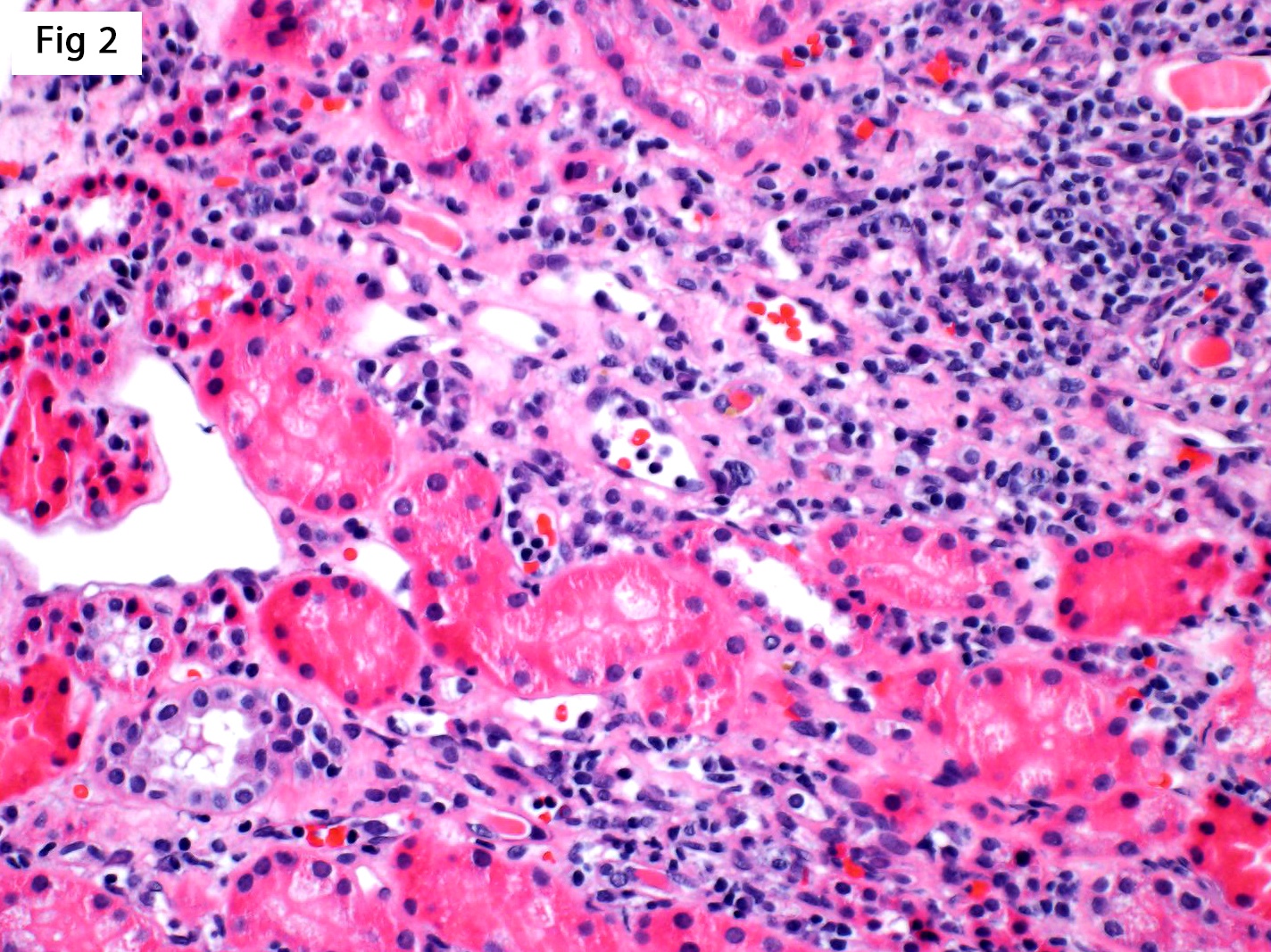
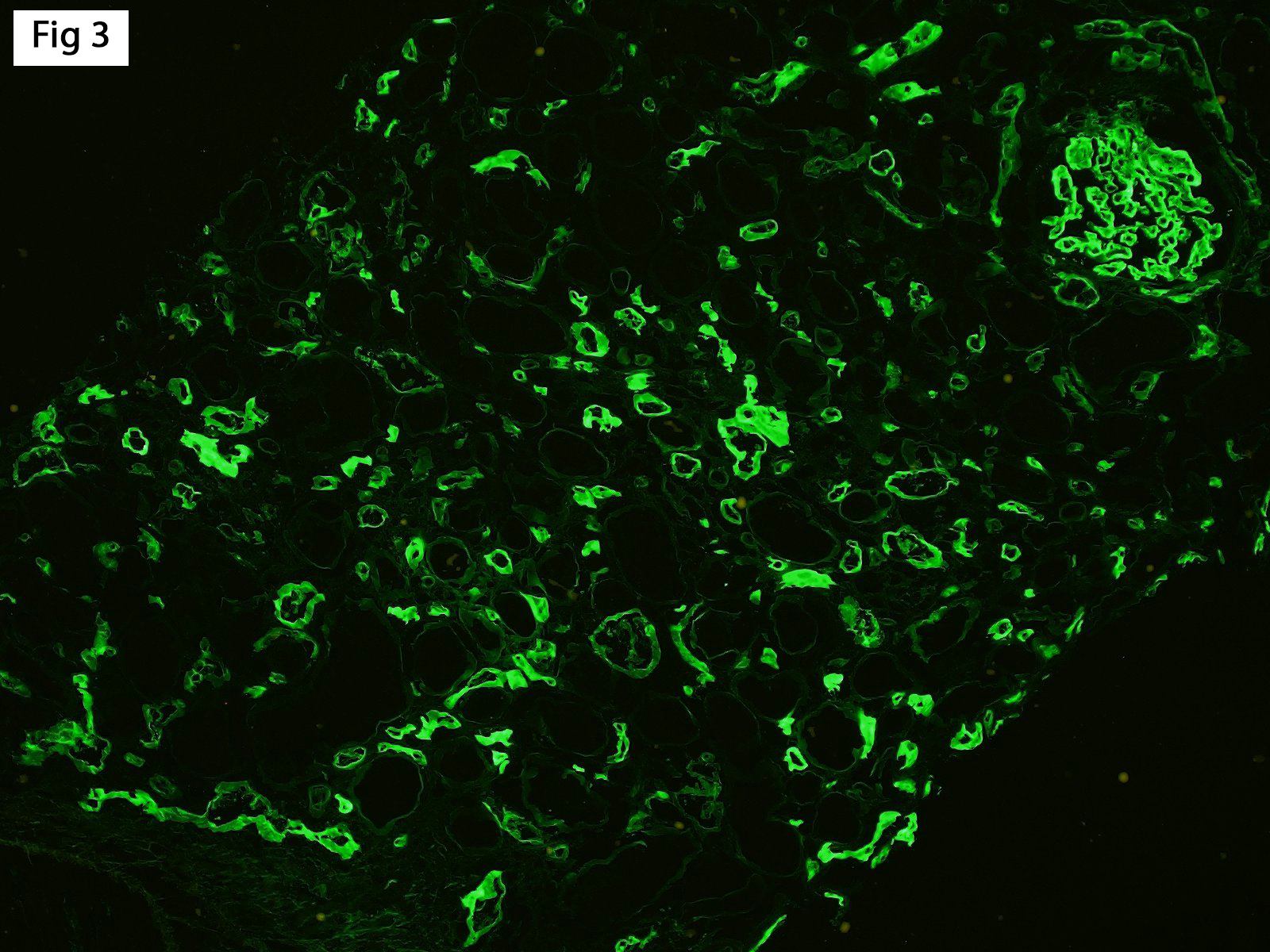
This biopsy was performed on a 37-year-old female with a history of type 1 diabetes mellitus, status post second deceased donor renal transplant, who now presents with allograft dysfunction (Cr 3.1 mg/dl) and mild proteinuria (UPC 1.1 g/g). No donor-specific antibody (DSA) data was available at the time of the biopsy. The biopsy shows severe glomerulitis and chronic transplant glomerulopathy (Fig 1), along with mild peritubular capillaritis (Fig 2) and diffusely positive C4d staining in peritubular capillaries (Fig 3). Based on the Banff 2017 kidney meeting report, this case can now be diagnosed as chronic active antibody-mediated rejection, and the term “suspicious for” should no longer be used. Of note, while DSA data is no longer required for the diagnosis of AMR when C4d is positive, the report still strongly suggests performing DSA testing on all cases meeting morphologic criteria for antibody-mediated rejection.
Reference: Haas M, et al. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am J Transplant. 2018; 18: 293-307.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.