
This biopsy came to us due to acute renal failure and proteinuria.
The patient was a gentleman in his late 70s, with elevated creatinine up to 2.0 mg/dl, and proteinuria quantified at about 1 gram per 24 hours. His serum albumin was remarkably low, at 2.5 g/dL. He was also anemic, with hemoglobin at 9.1 g/dL. ANCA serologies were positive and the patient had been treated with high doses of steroids for a few weeks prior to the biopsy. SPEP was negative for monoclonal proteins. ANA serology was negative.
Fortunately for us, the biopsy was a great sample of renal tissue, entirely represented by cortex, and already at low power, one could identify a very obvious cause for acute renal failure: widespread acute tubular injury.
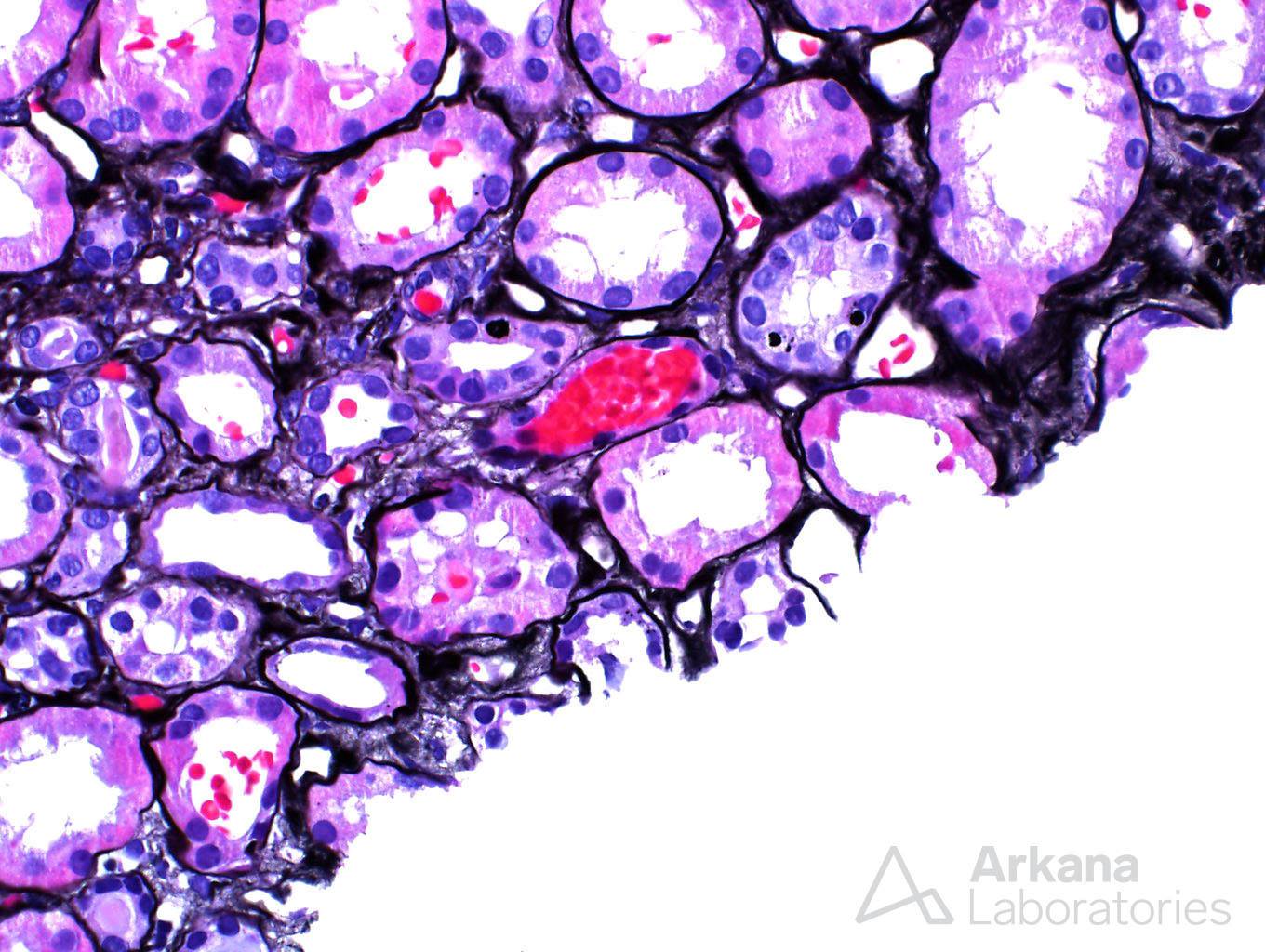
As one can see, the tubuli were definitely not “happy campers”. They were marked by tubular dilatation, and the proximal tubular cells were flattened, as opposed to their usual columnar/cuboidal appearance. Tubular nuclei often times had easily visible nucleoli, a sign of tubular injury. And the tubular brush border was effaced.
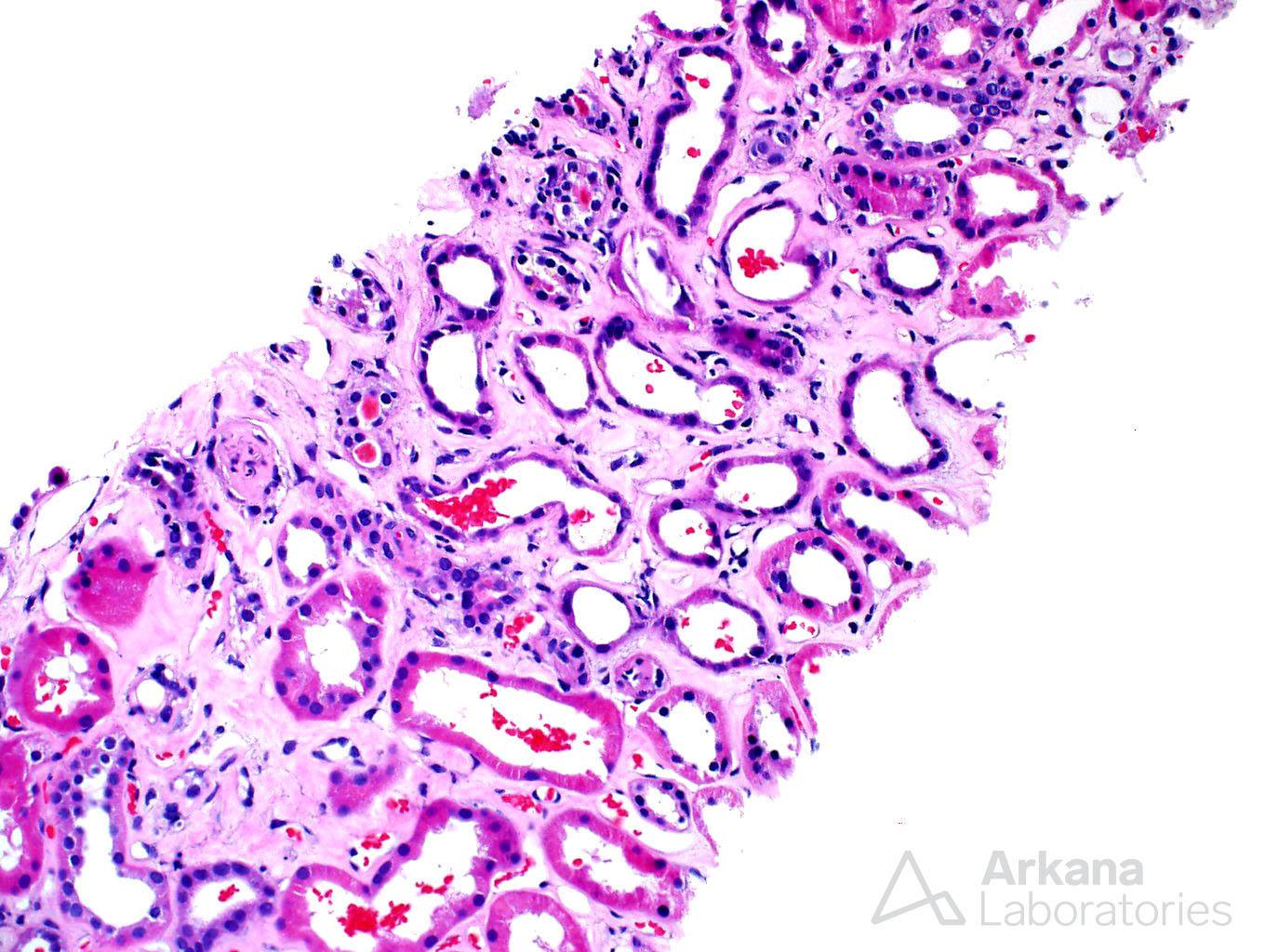
Interstitial inflammation was not a feature observed in the biopsy, and the possibility of interstitial nephritis was not a concern. However, a few tubules contained intratubular red blood cell casts.
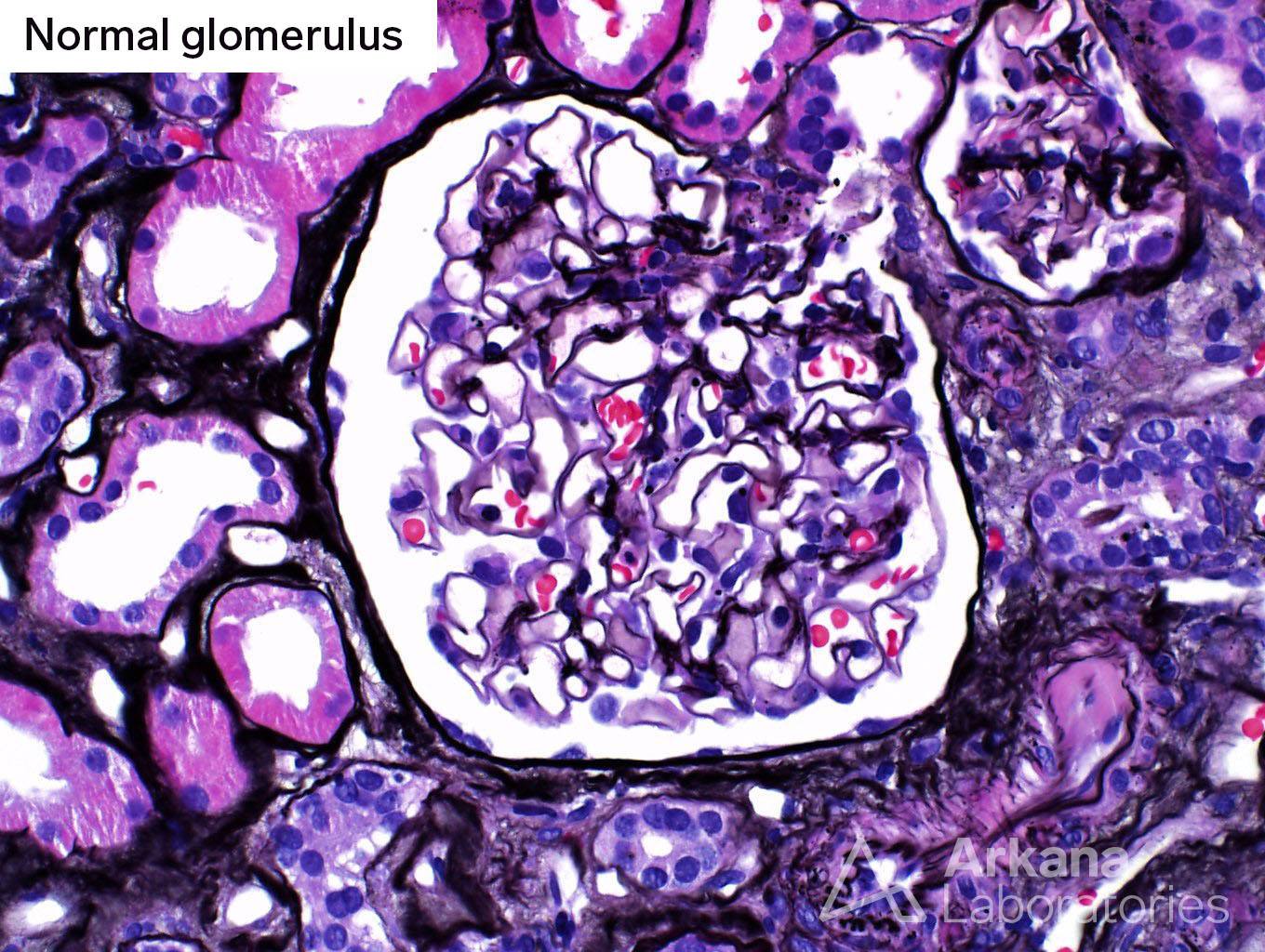
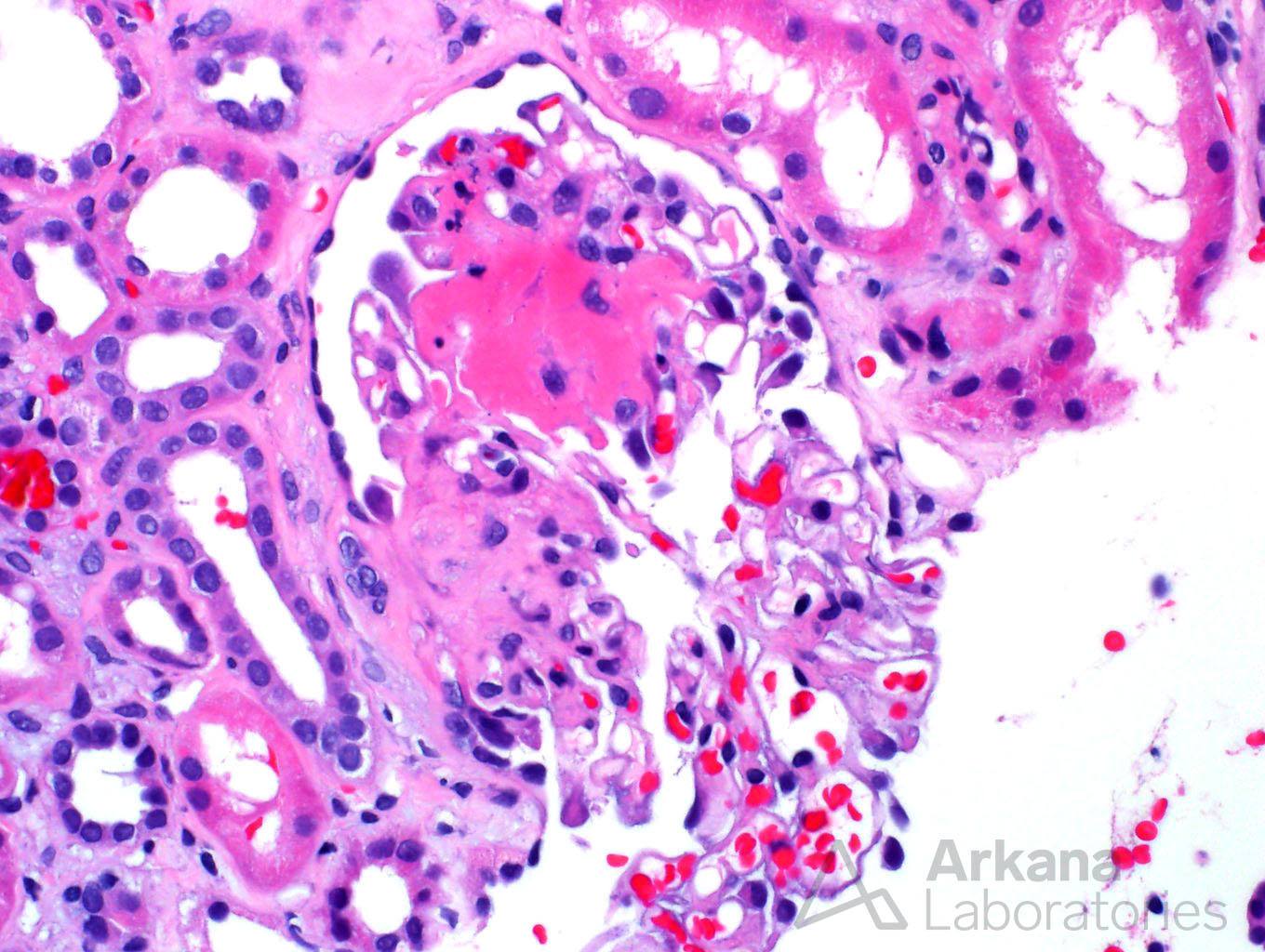
Glomeruli in the biopsy had a range of features. While some of the glomeruli had a fairly unremarkable appearance, other glomeruli showed an atypical pattern of segmental sclerosis, consistent with fibrous crescents.
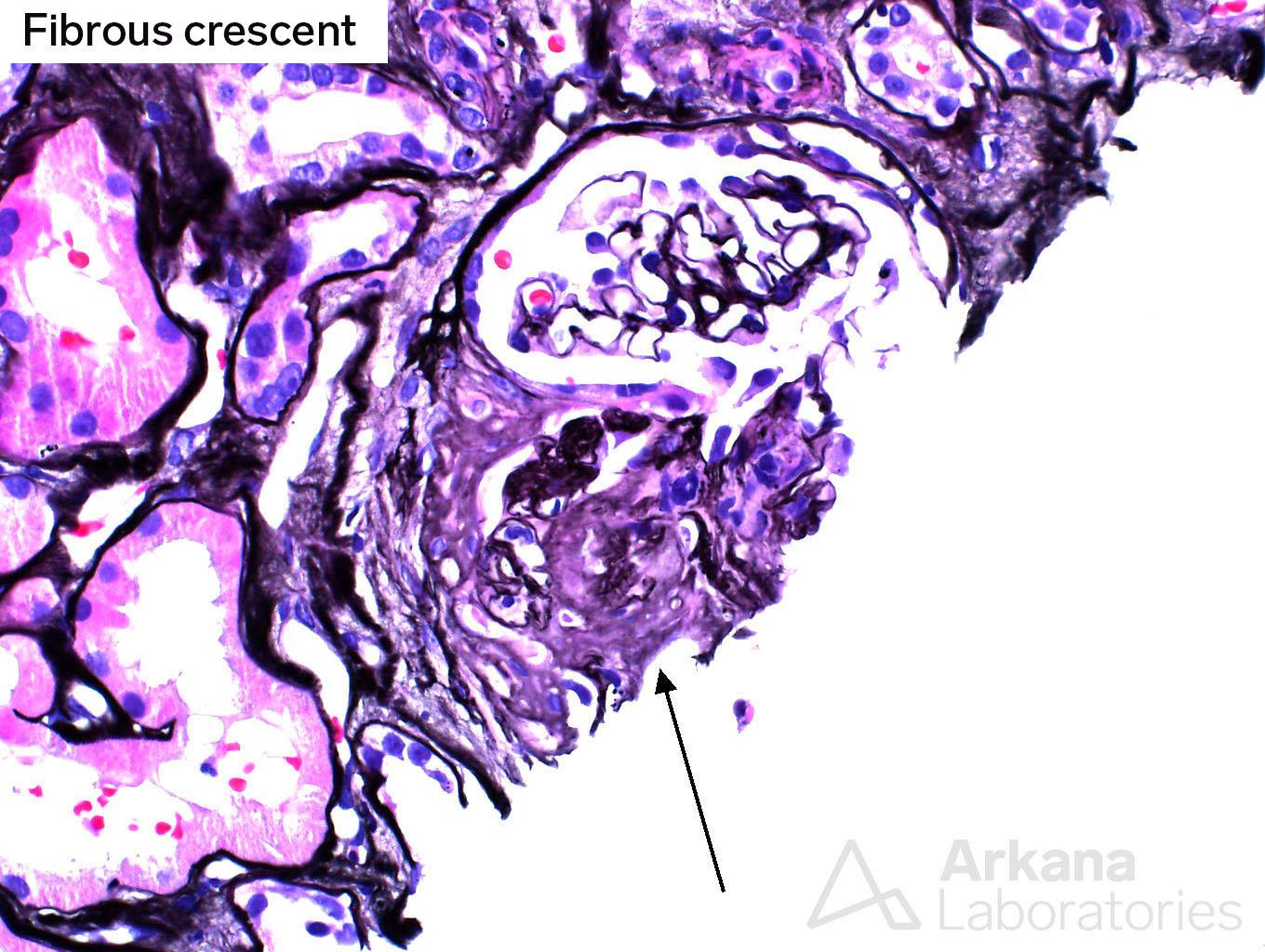
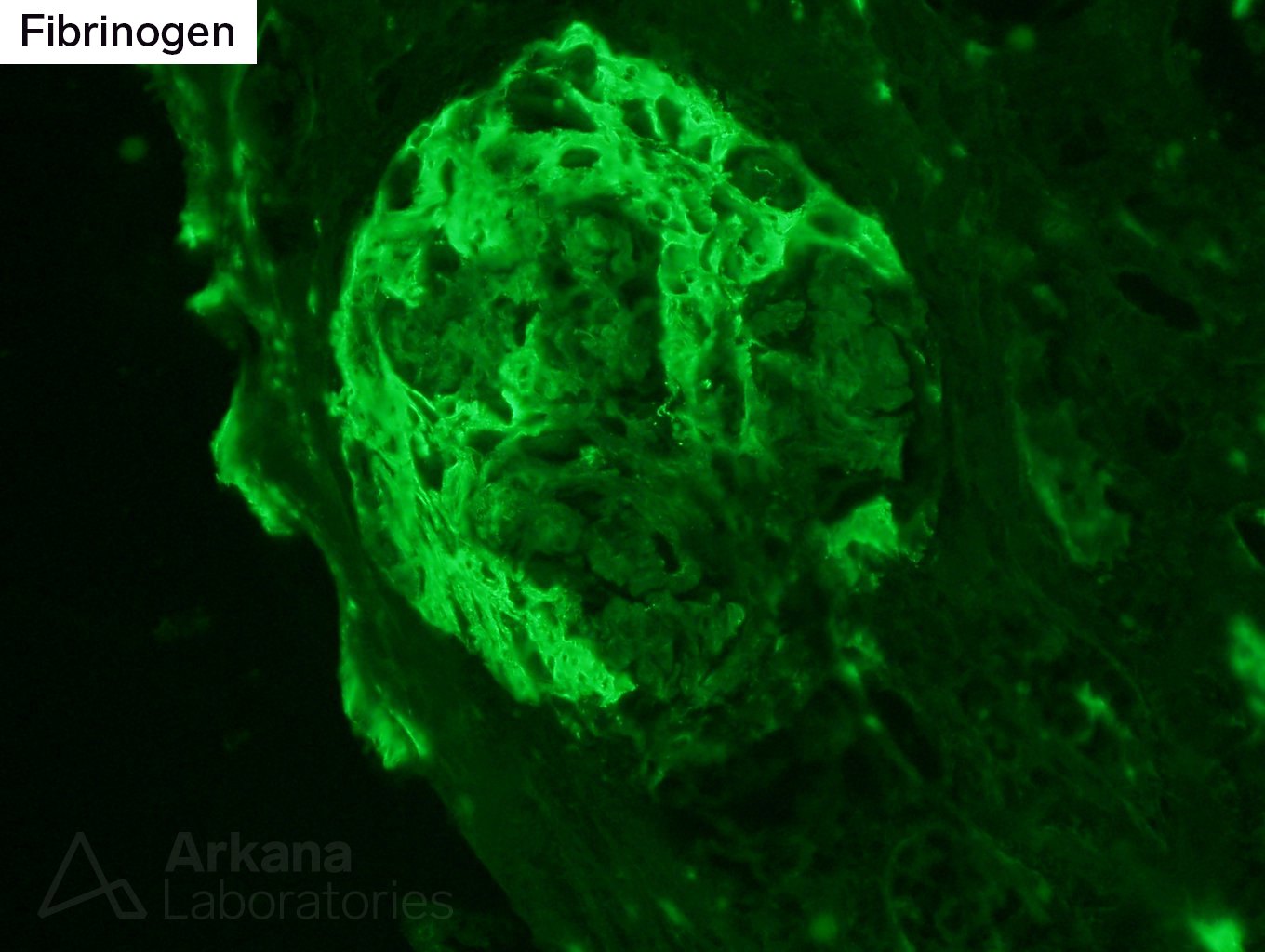
The presence of fibrous crescents represented scar formation in Bowman’s space after what was most likely a previous necrotizing lesion. This finding certainly was agreeable with the patient’s history of positive ANCA serologies and previous steroid therapy. In addition, fibrinogen staining within glomeruli was present on immunofluorescence studies, which were otherwise unremarkable and did not reveal any immune complex deposits.
At this point, one might decide that our findings represent acute tubular injury in a patient with sclerosing (or healed) crescentic glomerulonephritis. Nobody would be at fault if the pathologist reported that there was no activity on the renal biopsy, as pertaining to the glomerulonephritis/vasculitis process. After all, a good cortical sample was examined, and the reason for renal failure was well established. Chronic glomerular lesions could just prove that the patient’s therapy was effective.
However, some pieces of the puzzle were suspicious to our pathologist.
The first red flag was the presence of fresh red blood cell casts. These are usually a sign of active glomerulonephritis, and their significance is ominous, just as it would be on urine sediment.
The presence of fibrinogen staining was also unsettling. However, fibrinogen is a “sticky” stain and may be identified in chronic lesions, or sometimes even non-specifically.
With that worry in mind, we proceeded to dig deeper. In this case, quite literally, and deeper sections were examined.
A new set of slides was cut and stained with PAS and H&E stains. This choice of stains is based on the relative simplicity of the stains themselves, coupled with the combination of highlighting areas of necrosis (easily seen on H&E), and basement membranes (best seen on PAS). Within a mere hour of initially looking at the case, the pathologist had this new set of slides available for review.
The first sections did not look much different from what had been previously seen. However, at the 4th deeper section a glomerulus showed …fibrinoid necrosis!
This single glomerulus made a difference in the diagnosis, which now became a focal necrotizing glomerulonephritis. Steroids had contained but not completely solved the patient’s vasculitic process, as one would expect. Activity was still present, and the patient could potentially benefit from additional or more aggressive therapy.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.