
This biopsy came from a 70-year-old gentleman with acute renal failure. He had a known history of diabetes, hypertension, and chronic kidney disease. His baseline serum creatinine is between 1.7 mg/dl and 1.9 mg/dl and was found to be elevated up to 2.9 mg/dl. Proteinuria was quantified as 0.2 g/g on urine protein to creatinine ratio. Urinalysis showed trace blood and protein.
While processing the clinical information, one has to admit that this clinical presentation is not an unusual one. A fair number of patients will have a decline in renal function that reflects the reality of an already struggling kidney going into end-stage renal disease. Another group of patients has superimposed acute tubular injury on chronic changes of diabetes and hypertension. Finally, a smaller group have additional diagnoses, either glomerular disease or tubulointerstitial processes. Distinguishing which category an individual patient fits into best can be a clinical challenge; hence a renal biopsy may be of help.
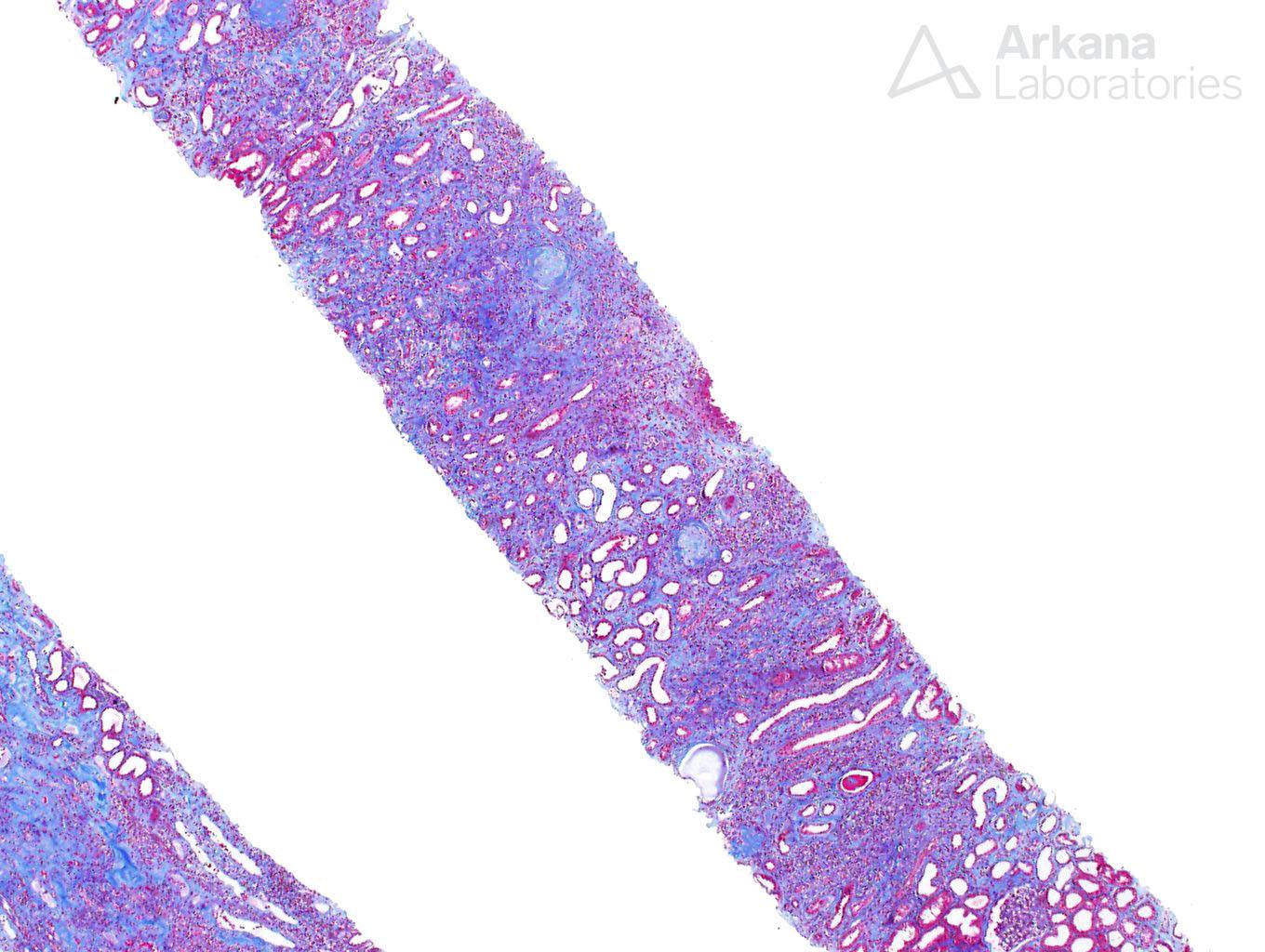
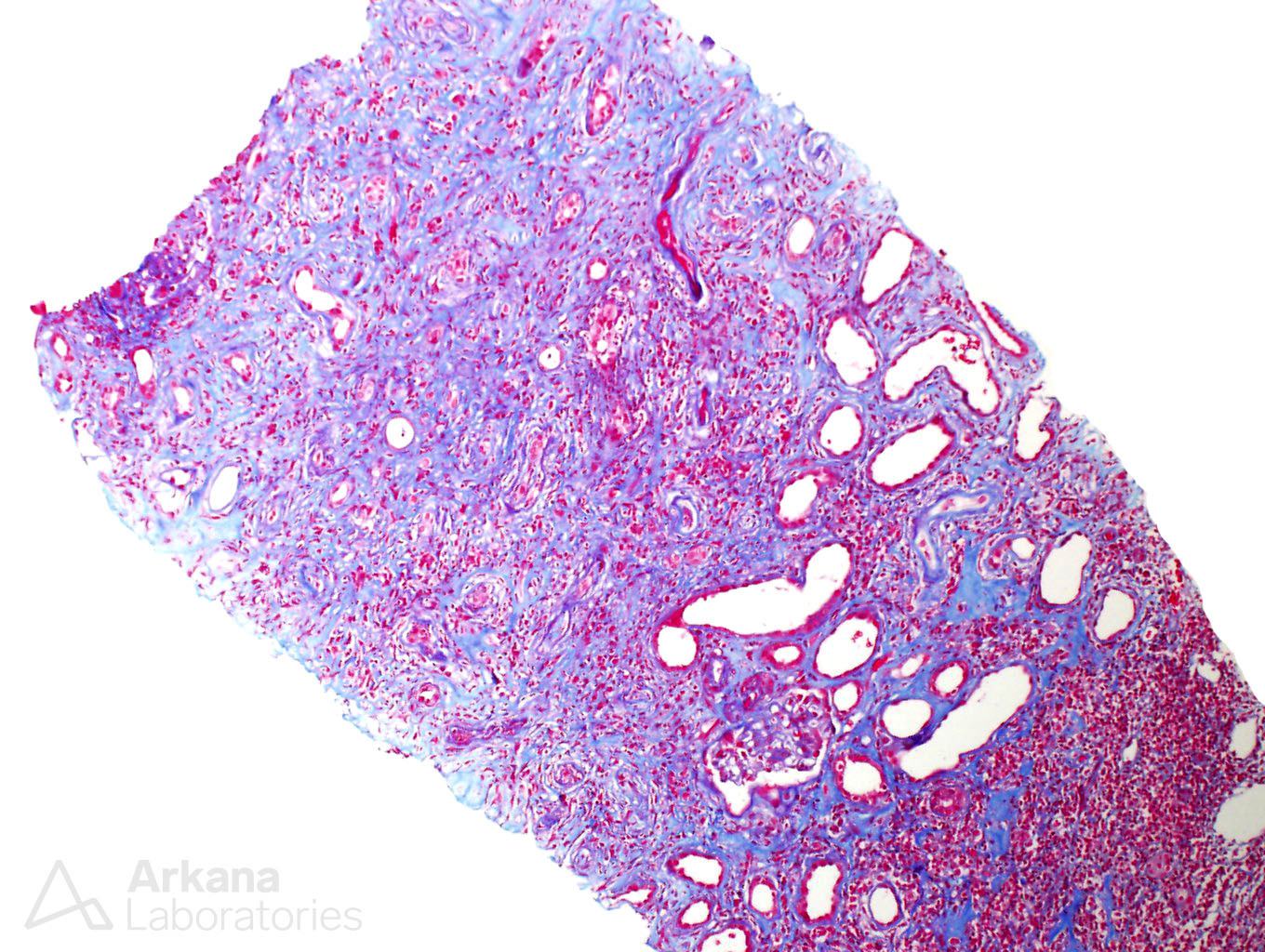
In our patient, the biopsy was marked by advanced chronicity, easily observed on low power sections, where the trichrome stain revealed a mostly blue background, indicative of widespread interstitial fibrosis.
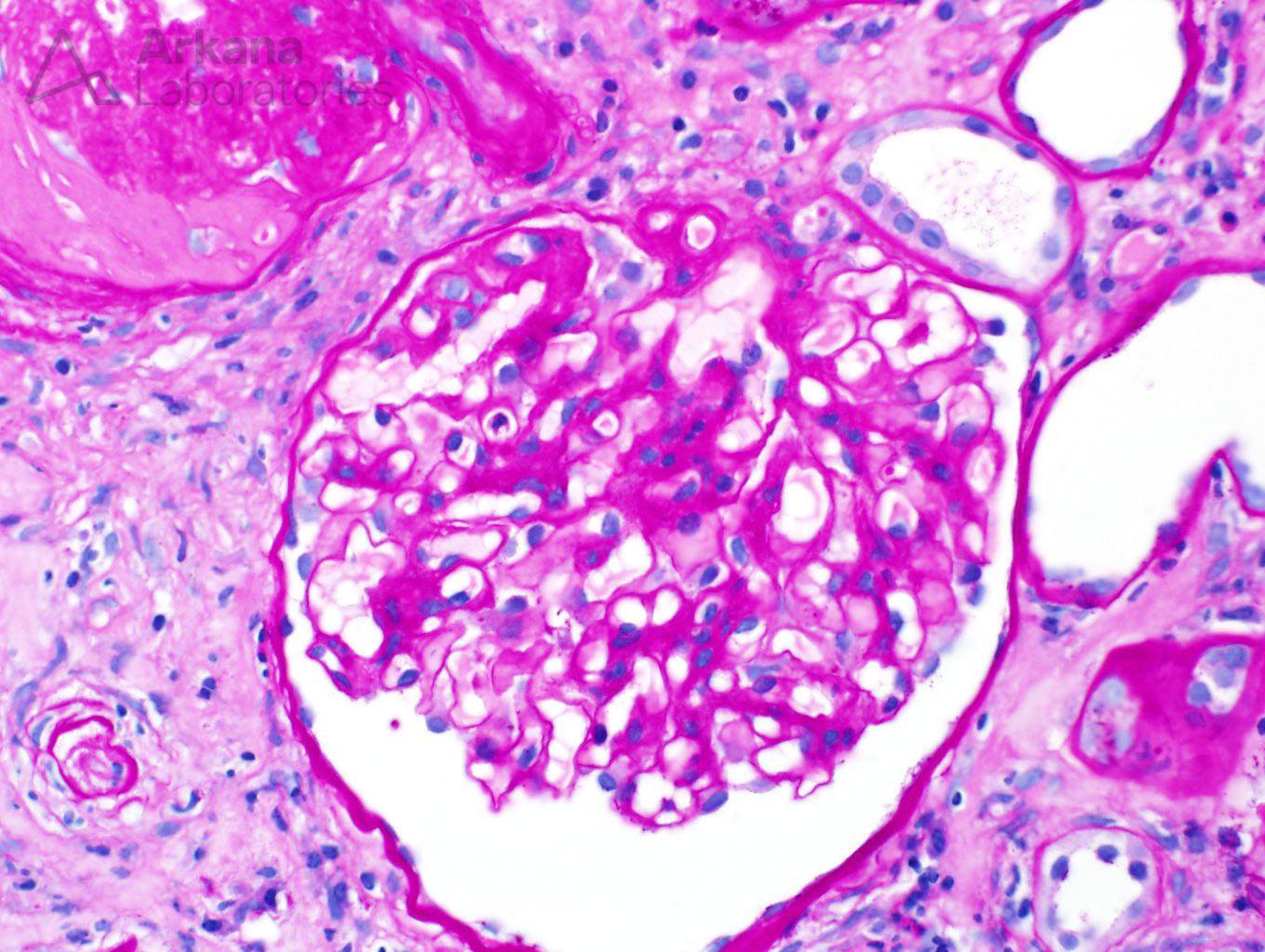
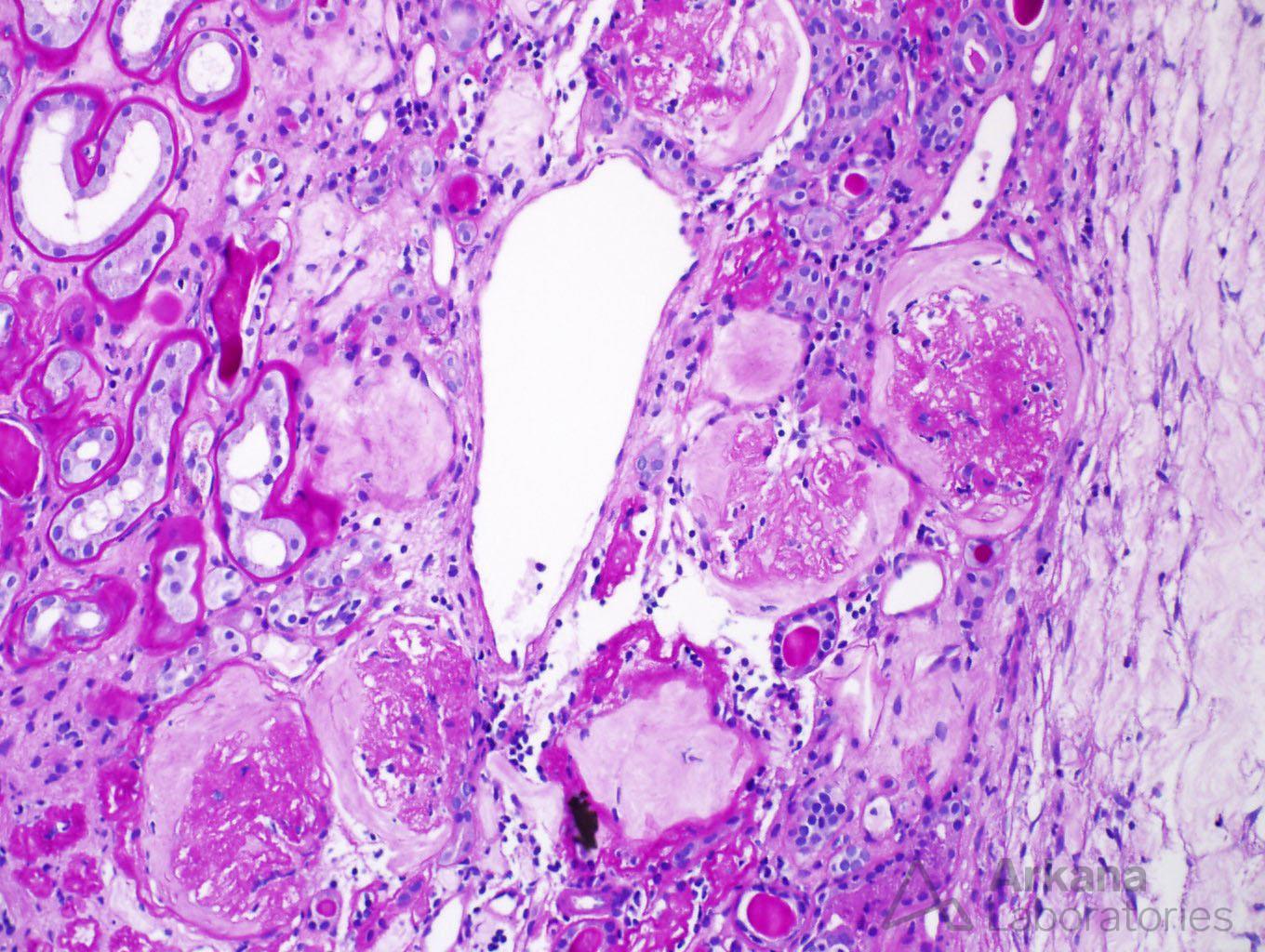
Changes of diabetic nephropathy were observed in the glomeruli, as mesangial expansion was diffusely present. Similar to the interstitial changes, the glomeruli showed significant chronicity as 18 of 23 glomeruli on the biopsy were globally sclerotic.
Overall, the case seemed to be a good fit for end-stage renal disease secondary to diabetic nephropathy. However, two features present on this biopsy caught the attention of our pathologist.
Within the biopsy, interstitial fibrosis was widespread, at about 80% of the cortex. However, some areas had a peculiar appearance. The fibrosis had a storiform pattern, also called “swirling” fibrosis. Within these areas of fibrosis, a number of plasma cells were present, along with lymphocytes.
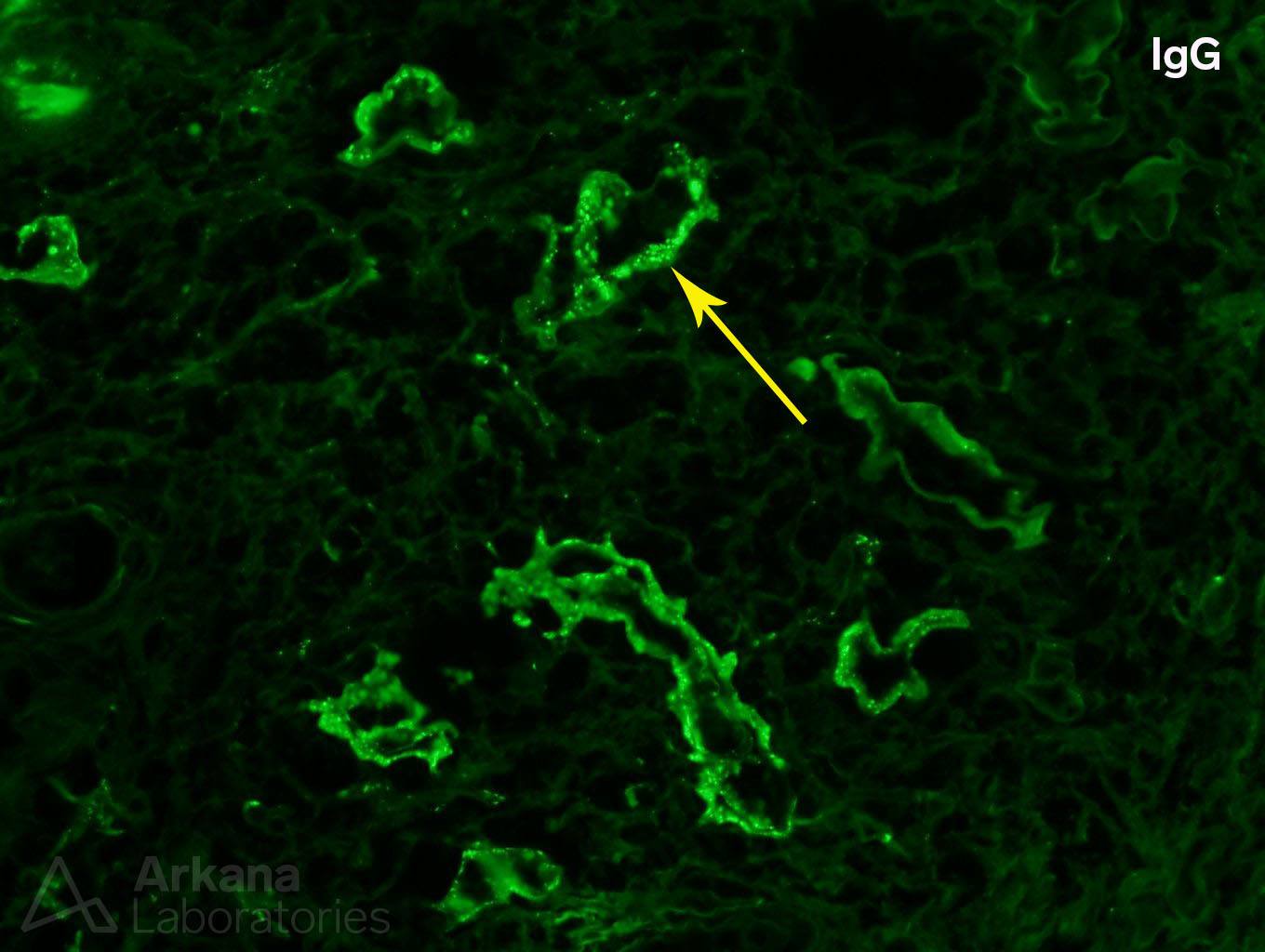
Another distinct finding was present on the immunofluorescence. Granular IgG deposits were identified along tubular basement membranes. Although patients with diabetes can have non-specific, linear staining of the tubular basement membranes with IgG, granular deposits are not a feature of diabetic nephropathy.
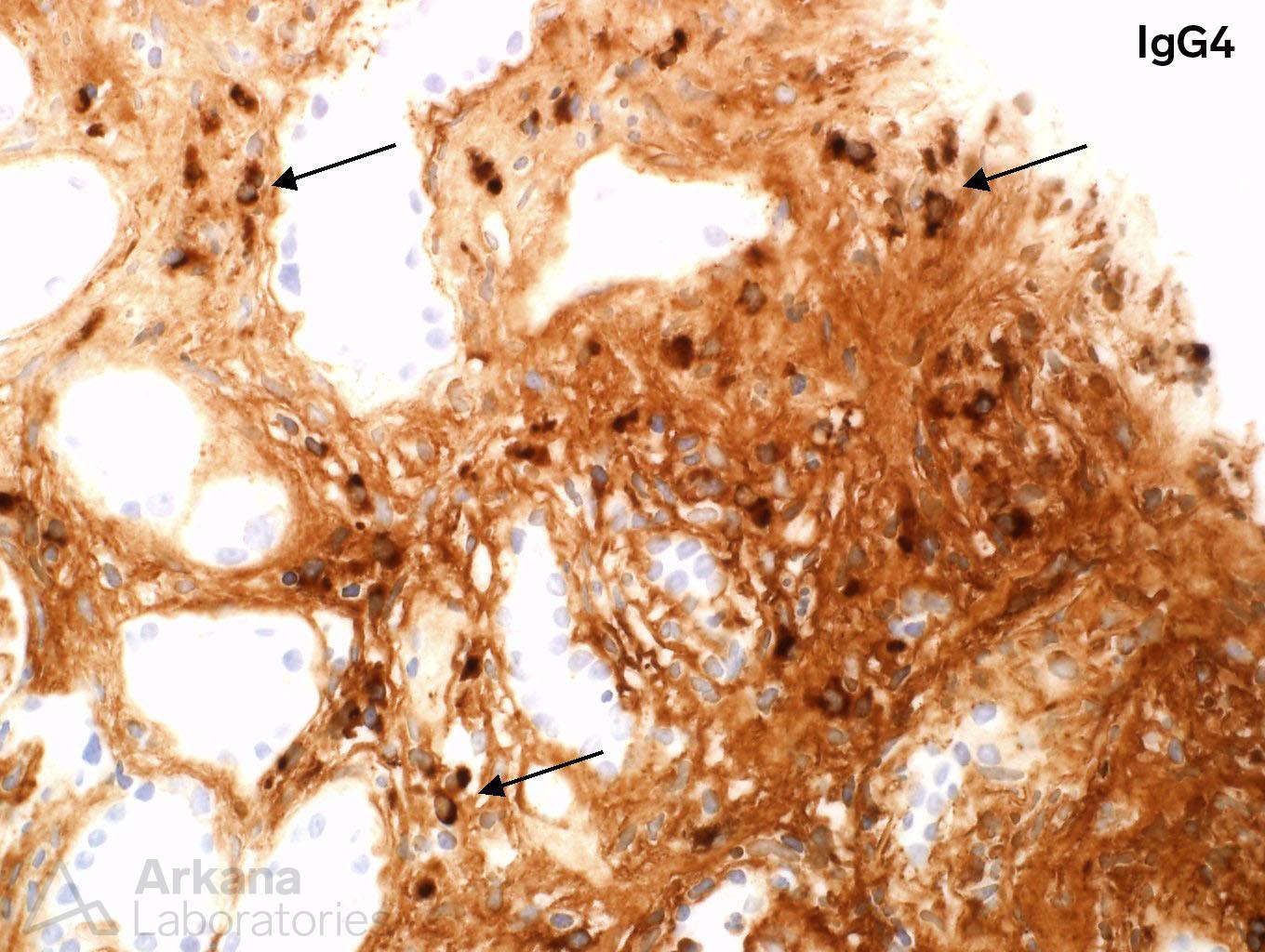
At this point, our pathologist decided that this biopsy deserved a bit more investigation. Digging deeper was in order, and an immunoperoxidase stain for IgG4 was performed. The IgG4 stain highlighted a large number of IgG4 positive plasma cells, within the interstitium, particularly in the areas of fibrosis.
With the results of IgG4 stain in hand, along with the other features in the biopsy, the diagnosis of IgG4-related disease was raised as a possibility. One cannot underscore enough the importance of this finding on a kidney biopsy, as IgG4-related disease can be treated, with often good clinical response, with immunosuppressive therapy. Additionally, IgG4-related disease has a patchy distribution, and even if the biopsy shows severe interstitial fibrosis, other areas of the kidney may be preserved. Finally, IgG4-related disease has other systemic manifestations as well and a diagnosis of IgG4-related disease in the kidney may help to elucidate other organ involvement, especially lacrimal and salivary glands, pancreas, and retroperitoneum.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.