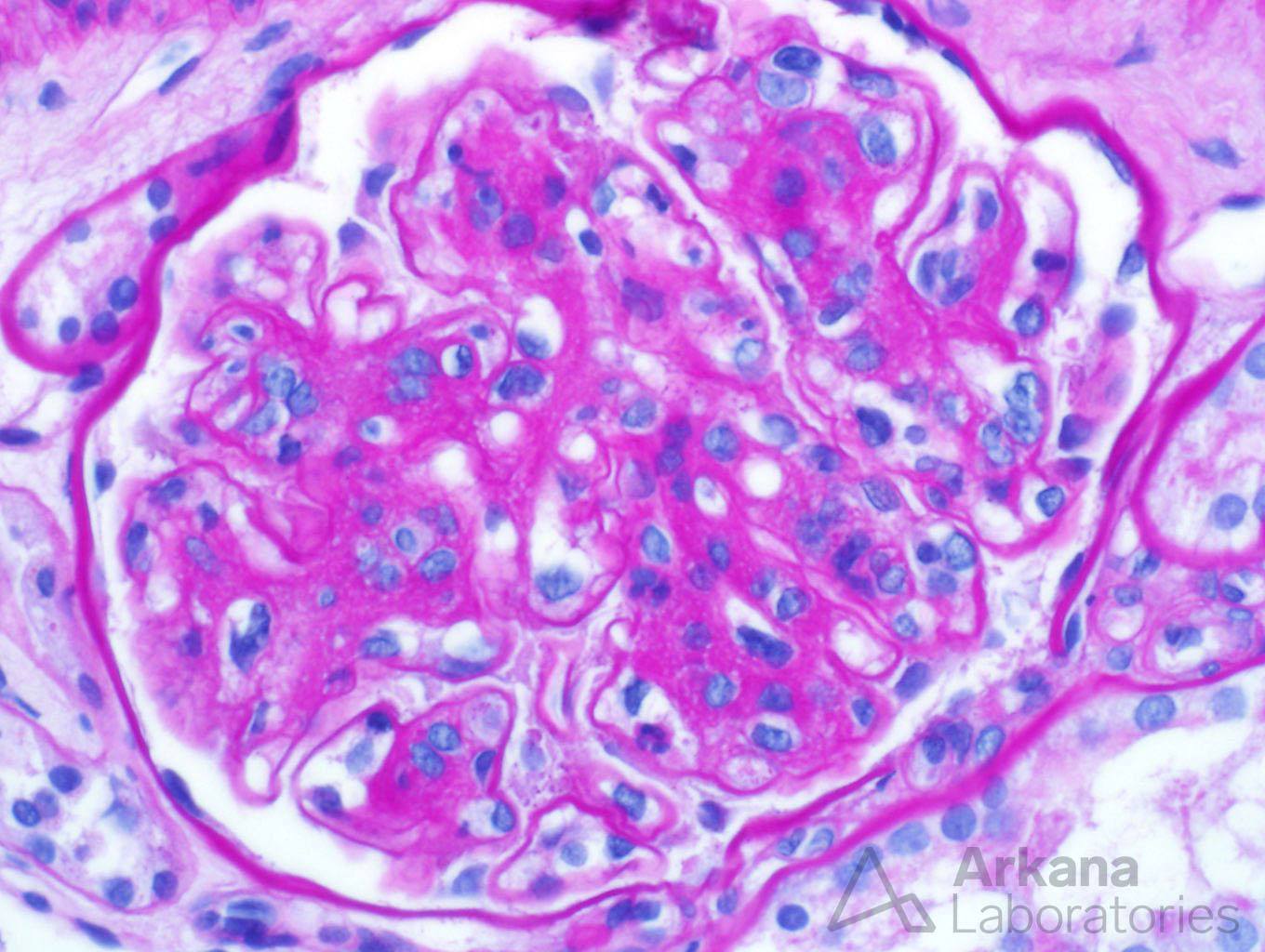
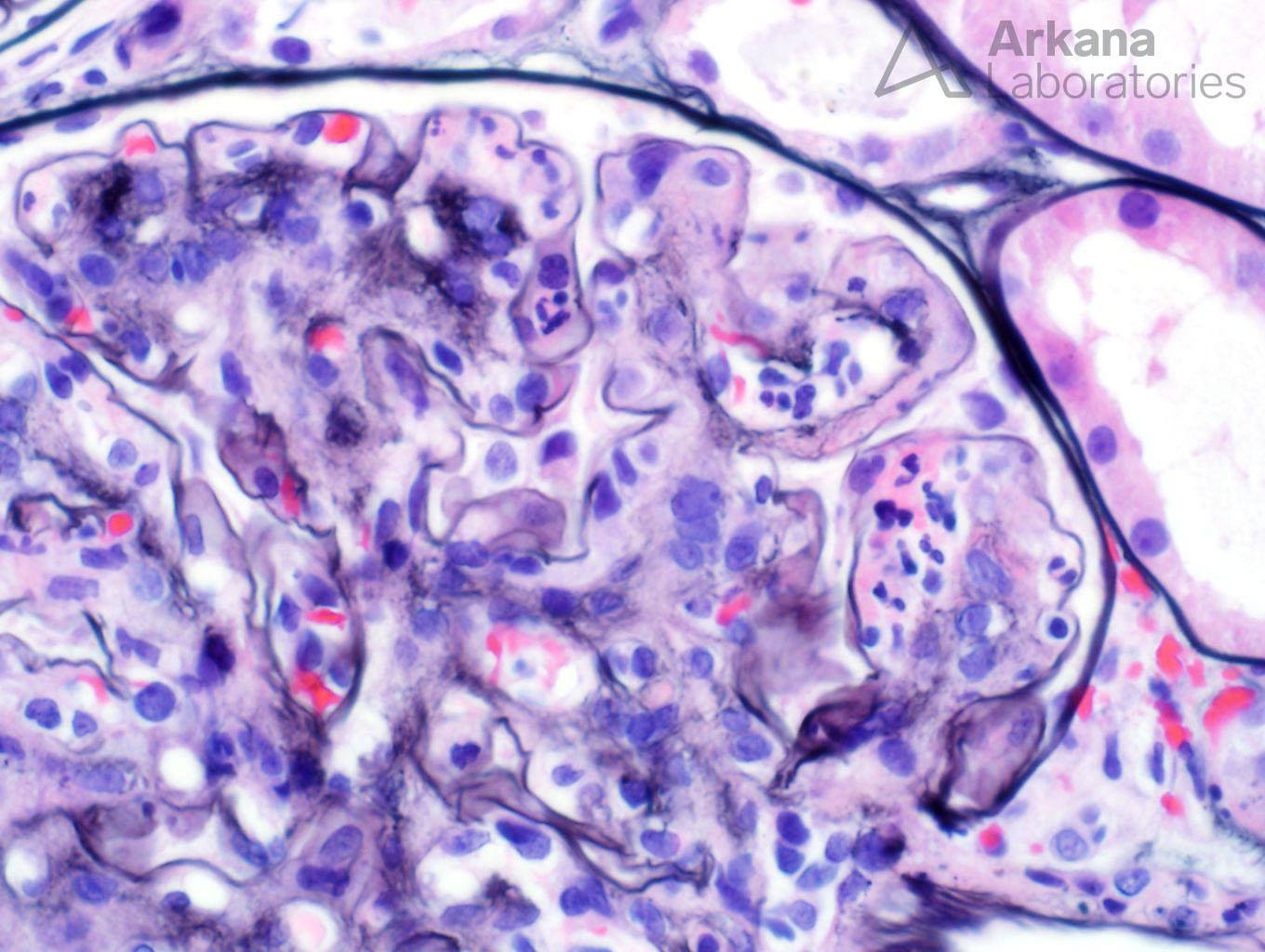
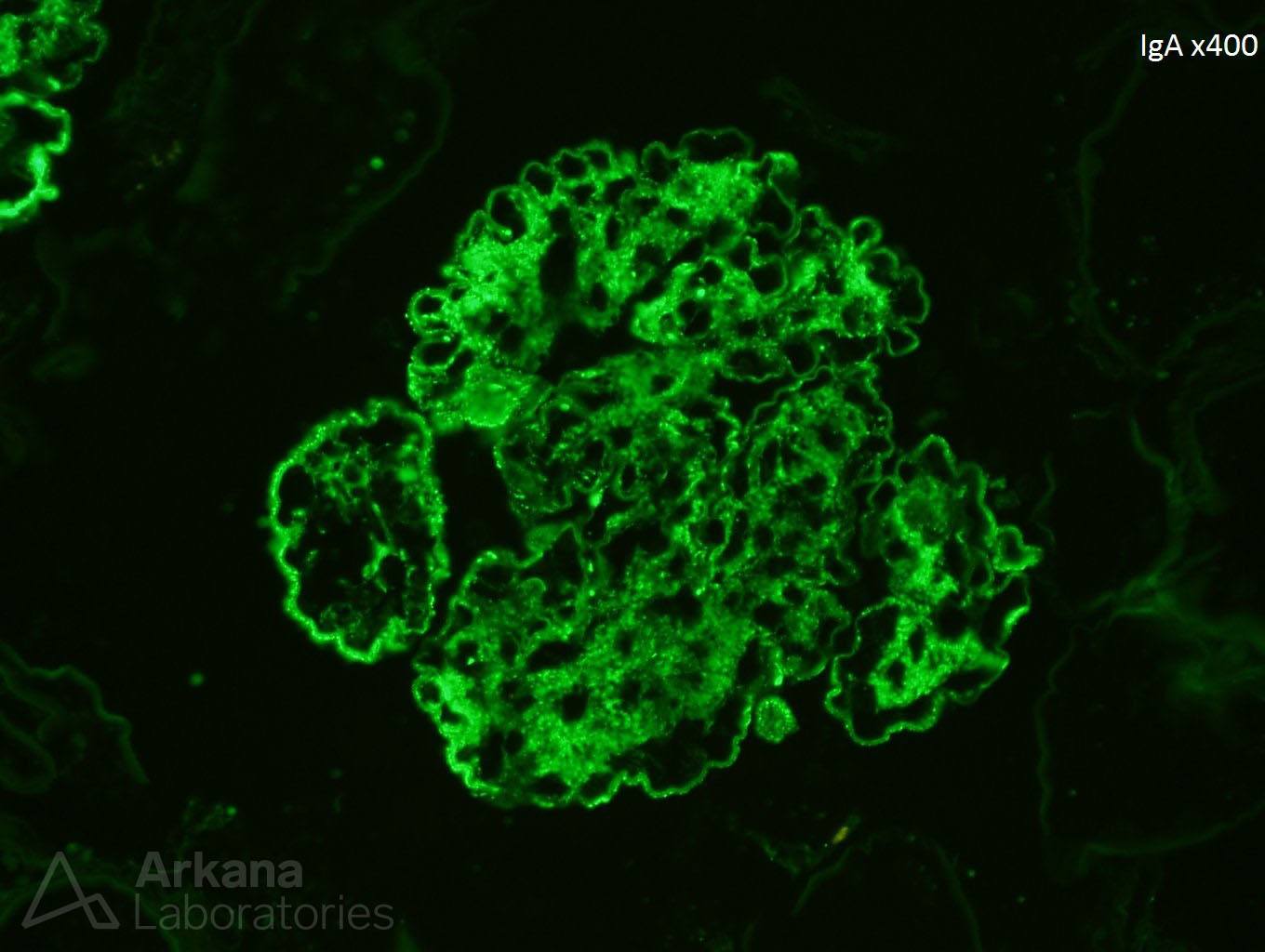
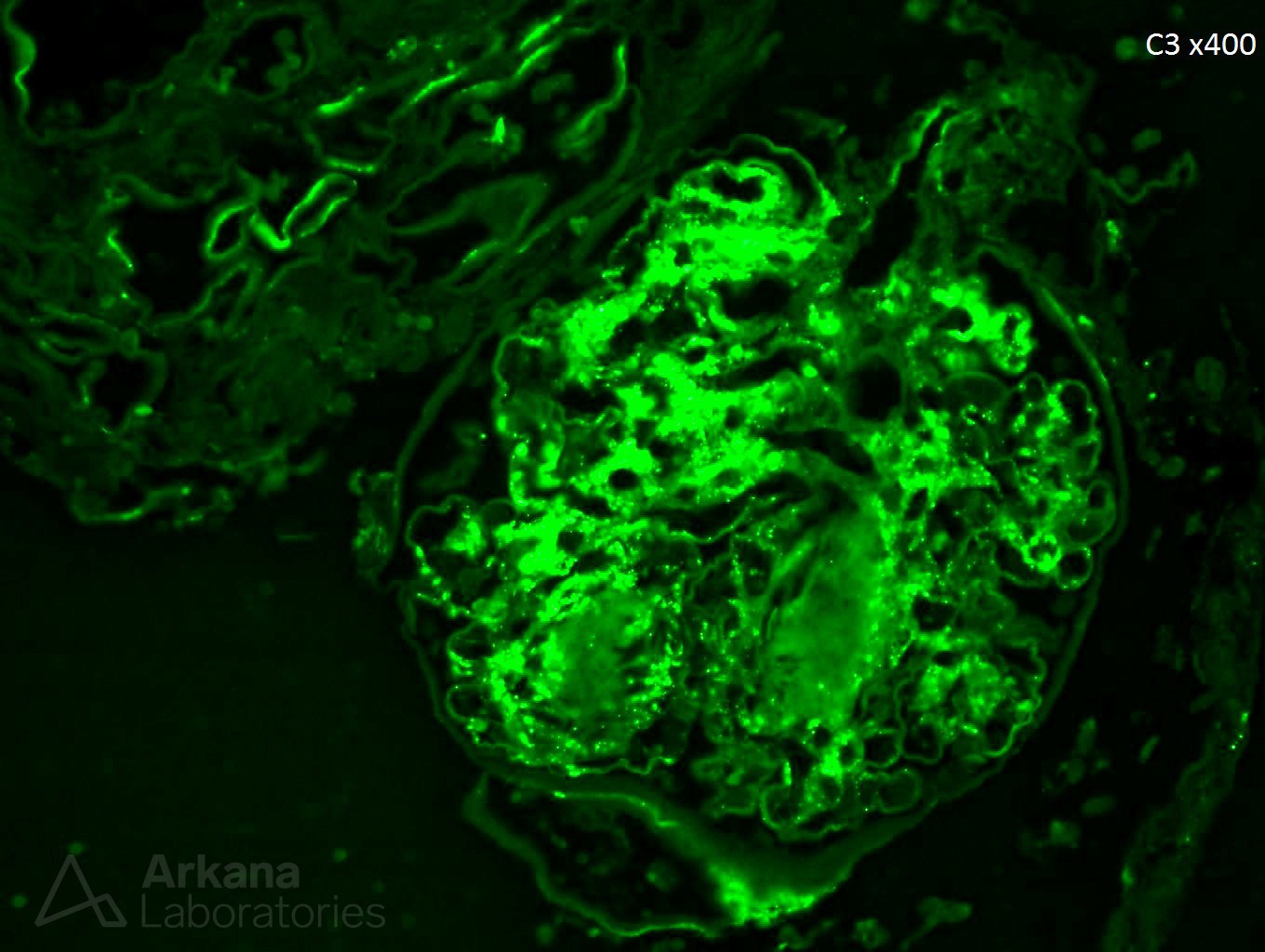
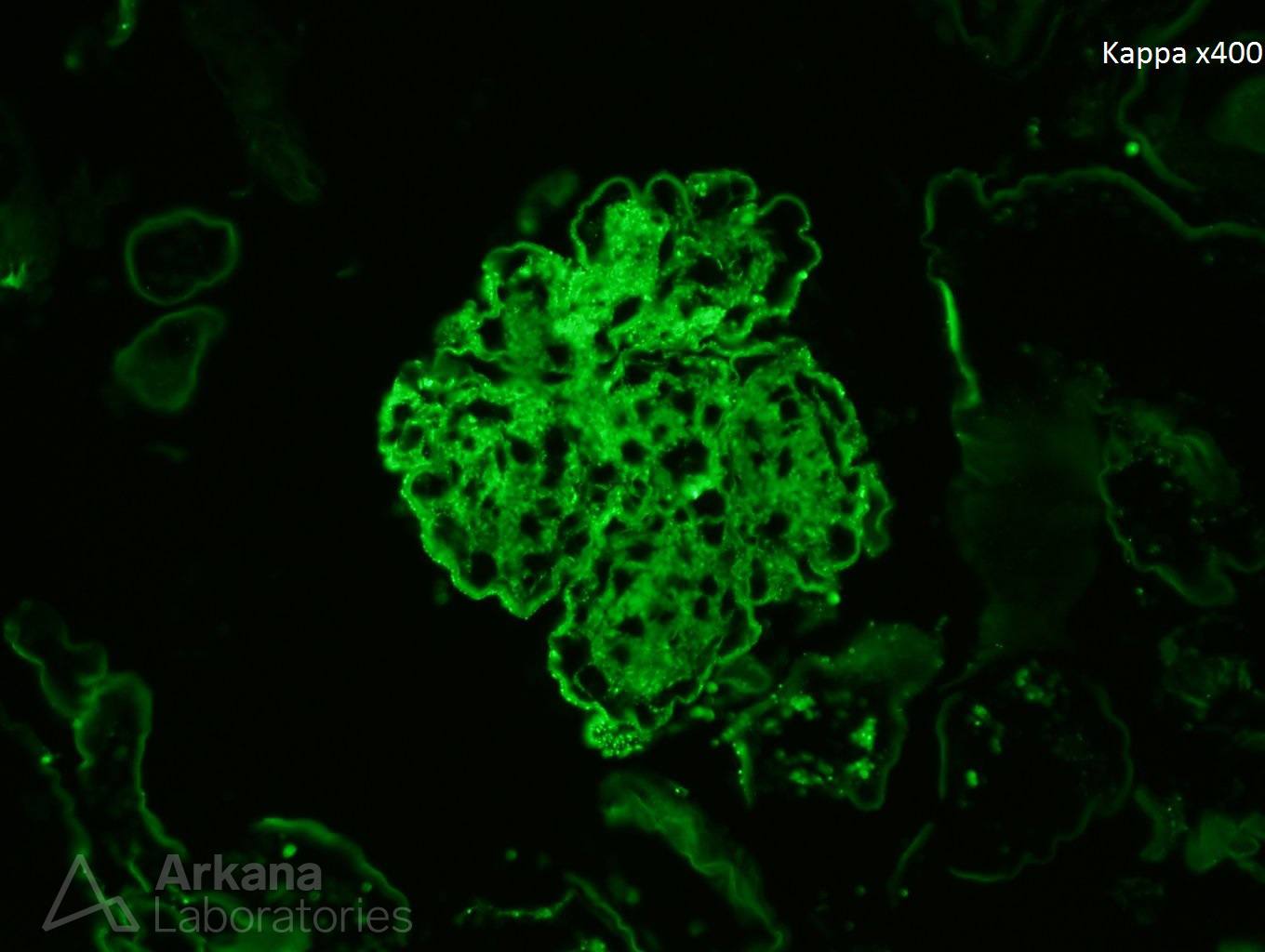
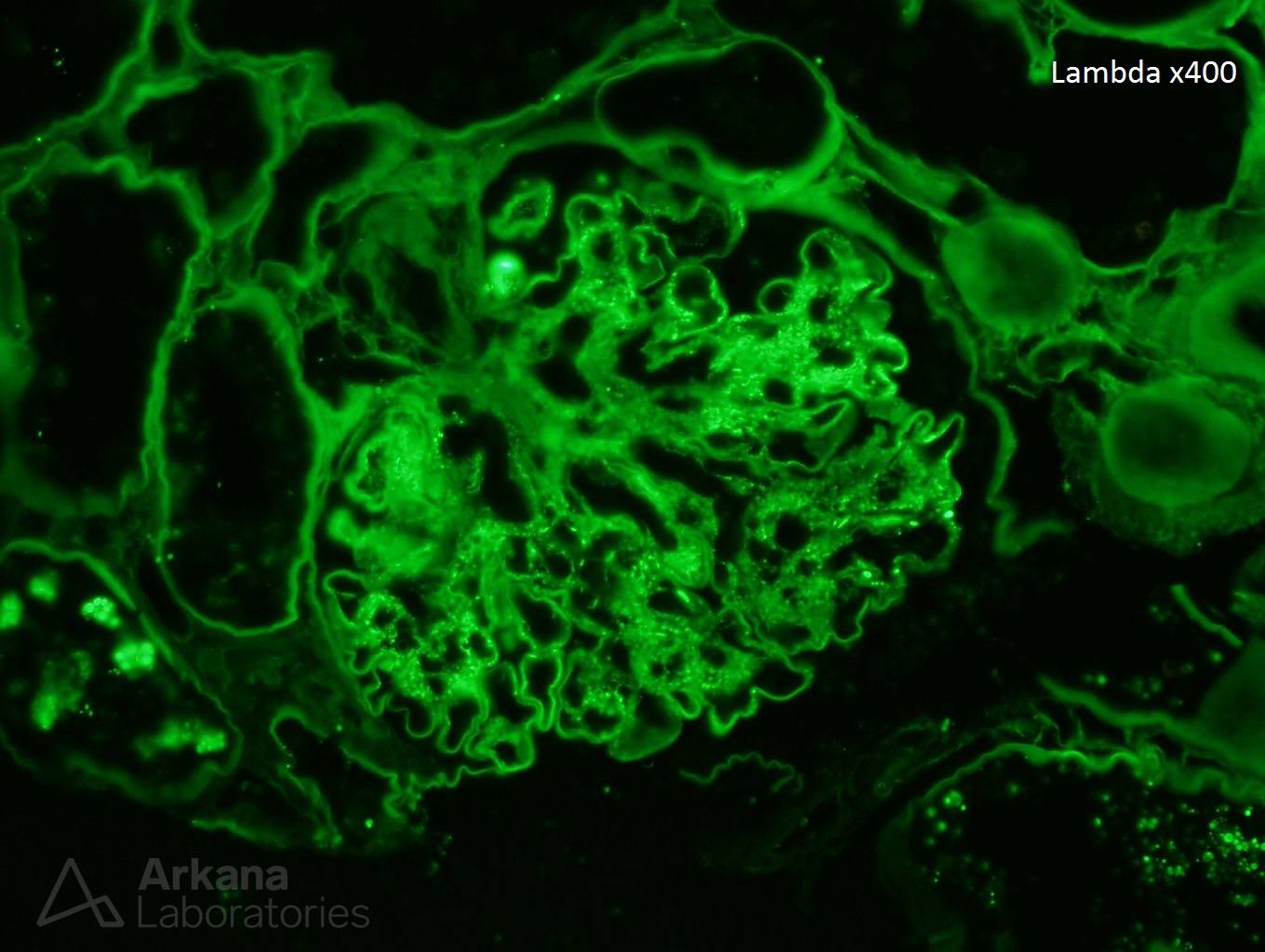
A 65-year-old male presents to the ER with a new onset rash and blood in his urine. The ER doc is worried about an allergic reaction and on chem 7 finds that the patient’s creatinine is 6.5 mg/dl. The patient has been a diabetic for over 20 years and had been diagnosed with cellulitis of his left foot a week ago by a family practice physician who gave him antibiotics. A skin biopsy of the new onset rash during this hospitalization shows a leukocytoclastic vasculitis with IgA deposition. A kidney biopsy is requested. The kidney biopsy shows nodular diabetic glomerulosclerosis (figure 1). On closer examination of the glomeruli, there is endocapillary hypercellularity and several neutrophils within the capillary lumens (figure 2). On immunofluorescence staining, there is strong granular staining of the capillary walls and mesangium with IgA (figure 3), C3 (figure 4), kappa (figure 5), and lambda (figure 6). The diagnosis of IgA dominant infection-associated glomerulonephritis is given.
IgA dominant infection-associated glomerulonephritis is an increasingly recognized morphological variant of glomerulonephritis which typically presents in older patients. Diabetes is a major risk factor and Staphylococcus infection is usually related to this entity. It is speculated that staphylococcal enterotoxins behave as superantigens which cause T-cell activation and subsequent cytokine burst. The cytokines are believed to activate B cells which produce polyclonal IgA and IgG which eventually result in immune complex deposition within the glomeruli. A few non-staphylococcal pathogens such as Pseudomonas aeruginosa, E. coli, Haemophilus influenza, and K. pneumonia have also been associated with IgA dominant infection-associated glomerulonephritis and in animal models can induce glomerular deposition of IgA and C3. Patients typically present with severe renal failure, proteinuria, and hematuria. A few histological clues to the diagnosis of this entity are proliferation (endocapillary neutrophils) within the glomeruli and bright C3 immunofluorescence stain. Prognosis is guarded with less than a fifth of patients fully recovering renal function.
https://www.ncbi.nlm.nih.gov/pubmed/21659781
https://www.ncbi.nlm.nih.gov/pubmed/21545311
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.