A 75-year-old Hispanic male presents with a creatinine of 3. His creatinine has slowly been creeping up over the last year from 1.8 to the current level. No hematuria or proteinuria is reported. Serologies for ANA, dsDNA, rheumatoid factor, hepatitis B, hepatitis C, and ASO are negative. Complement levels are normal. SPEP and UPEP are within normal limits.
What is the best diagnosis?
A. Arterionephrosclerosis
B. Amyloidosis, AL-Type
C. Amyloidosis, AA-Type
D. Amyloidosis, ALect2-Type
The best answer is D (Amyloidosis, ALect2-Type).
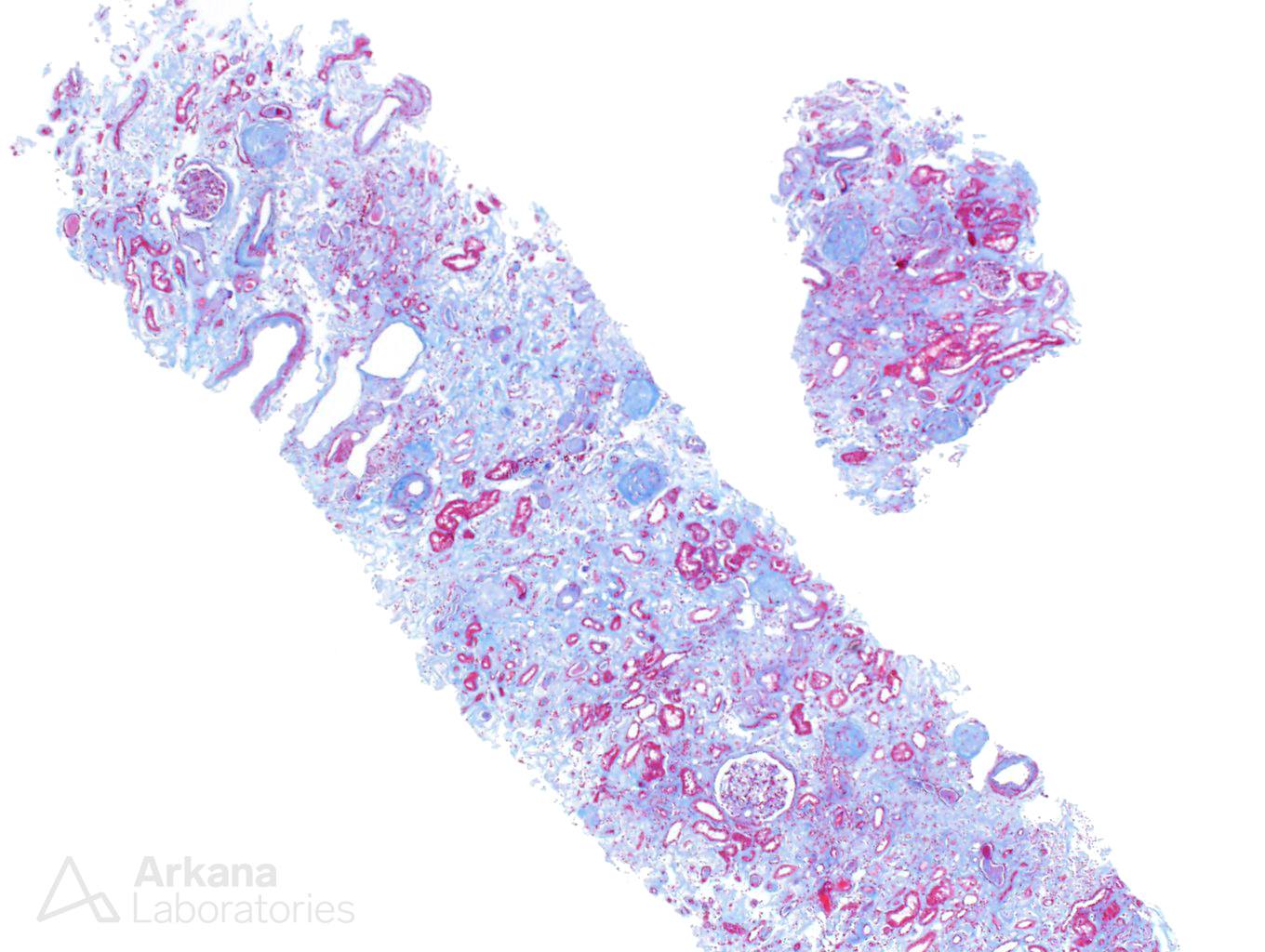
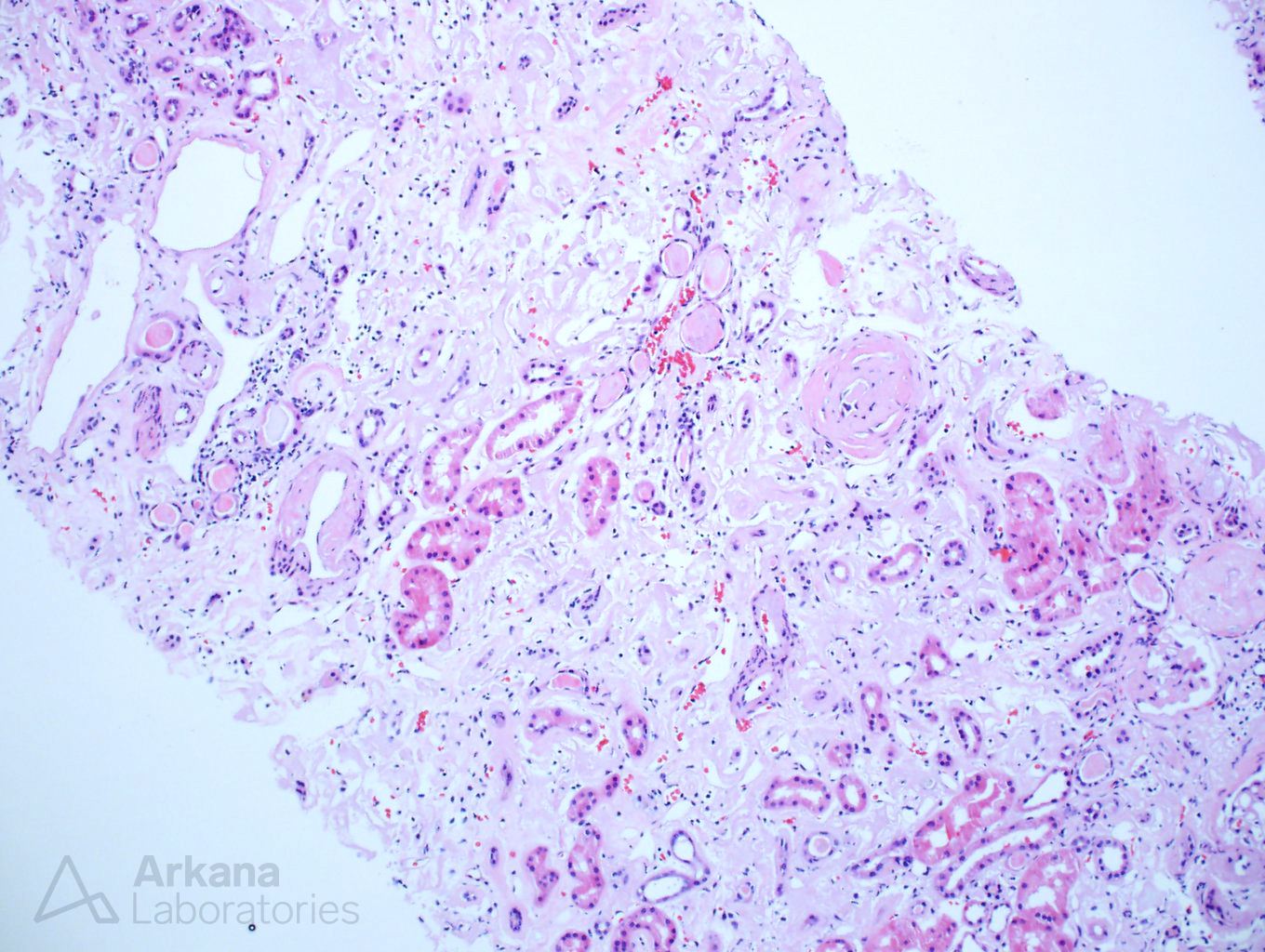
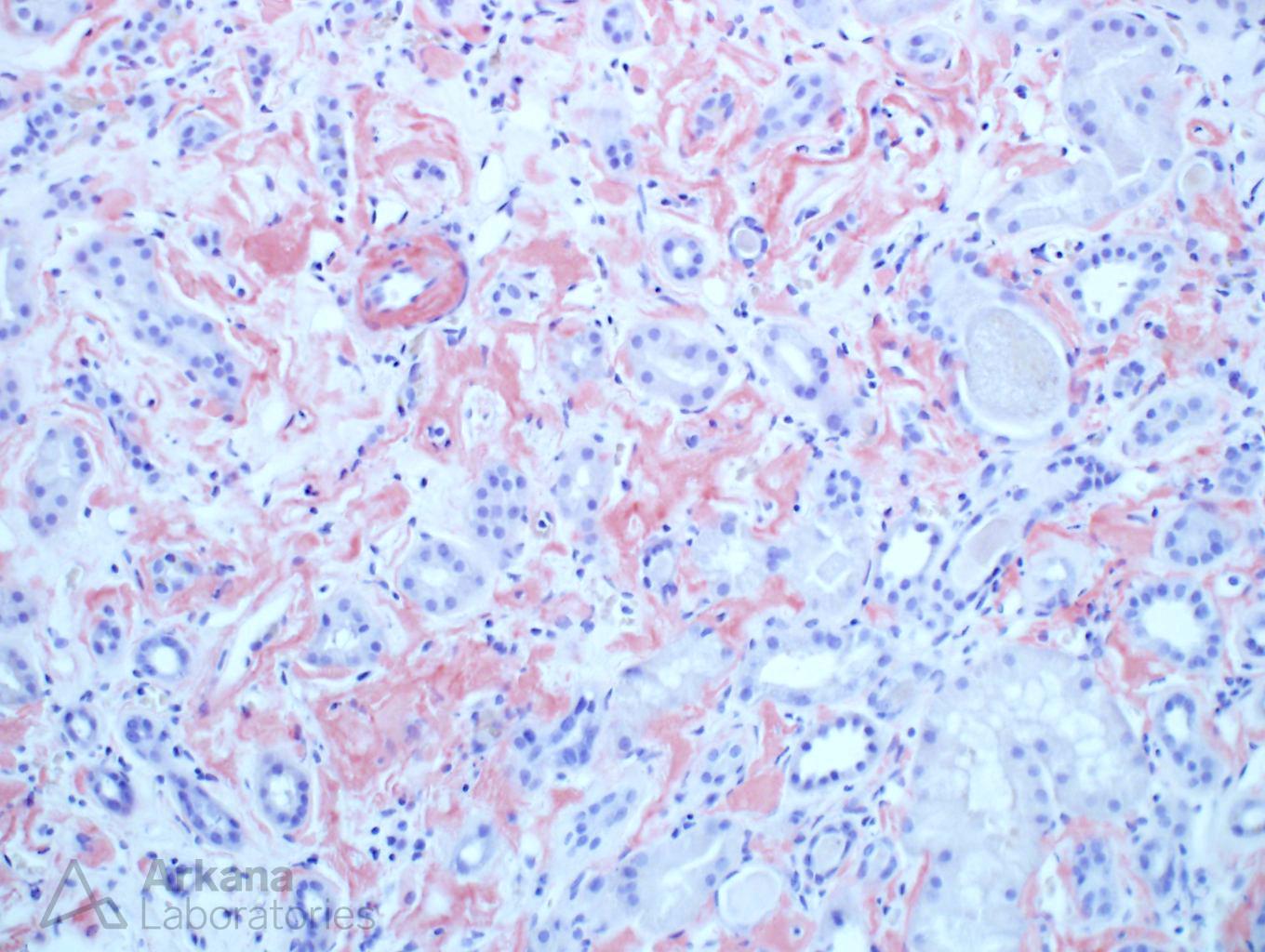
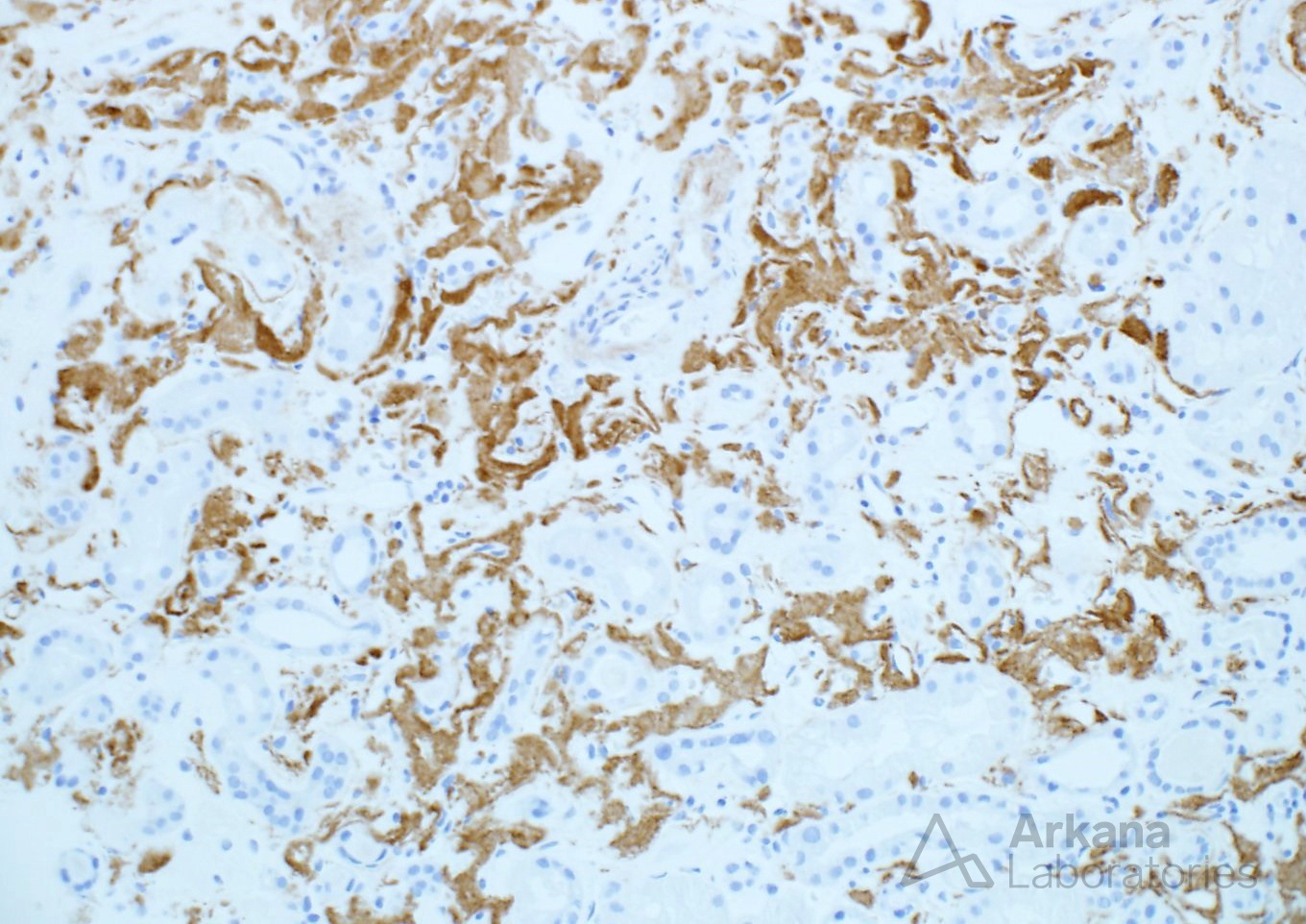
From low power, the glomeruli have an ischemic appearance and the arteries have severe arteriosclerosis. However, the Congo red stain is positive confirming the presence of amyloid. The normal levels of SPEP/UPEP help rule out AL-type amyloidosis and the immunofluorescence for kappa and lambda was equivocal. AA-type amyloidosis has a different pattern of deposition and usually affects the glomeruli. The pattern of distribution, Hispanic heritage, and positive immunoperoxidase staining for ALect2 confirm the diagnosis.
Reference: Larsen CP, Kossmann RJ, et al. Clinical Morphologic and Genetic Features of Renal Leukocyte Chemotactic Factor 2 Amyloidosis Kidney Int 2014 (2):378-82.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.