A diagnosis of chronic active antibody-mediated rejection (ABMR) requires morphologic evidence of chronic tissue injury (e.g. transplant glomerulopathy), evidence of current or recent antibody interaction with the vascular endothelium (e.g. linear C4d staining of peritubular capillaries), and serologic evidence of donor specific antibody (DSA) formation. Importantly, the revised 2017 Banff classification of ABMR and T cell-mediated rejection (TCMR) recognizes C4d positivity as a substitute for DSA for diagnosing ABMR, although DSA testing is still strongly encouraged (see reference).
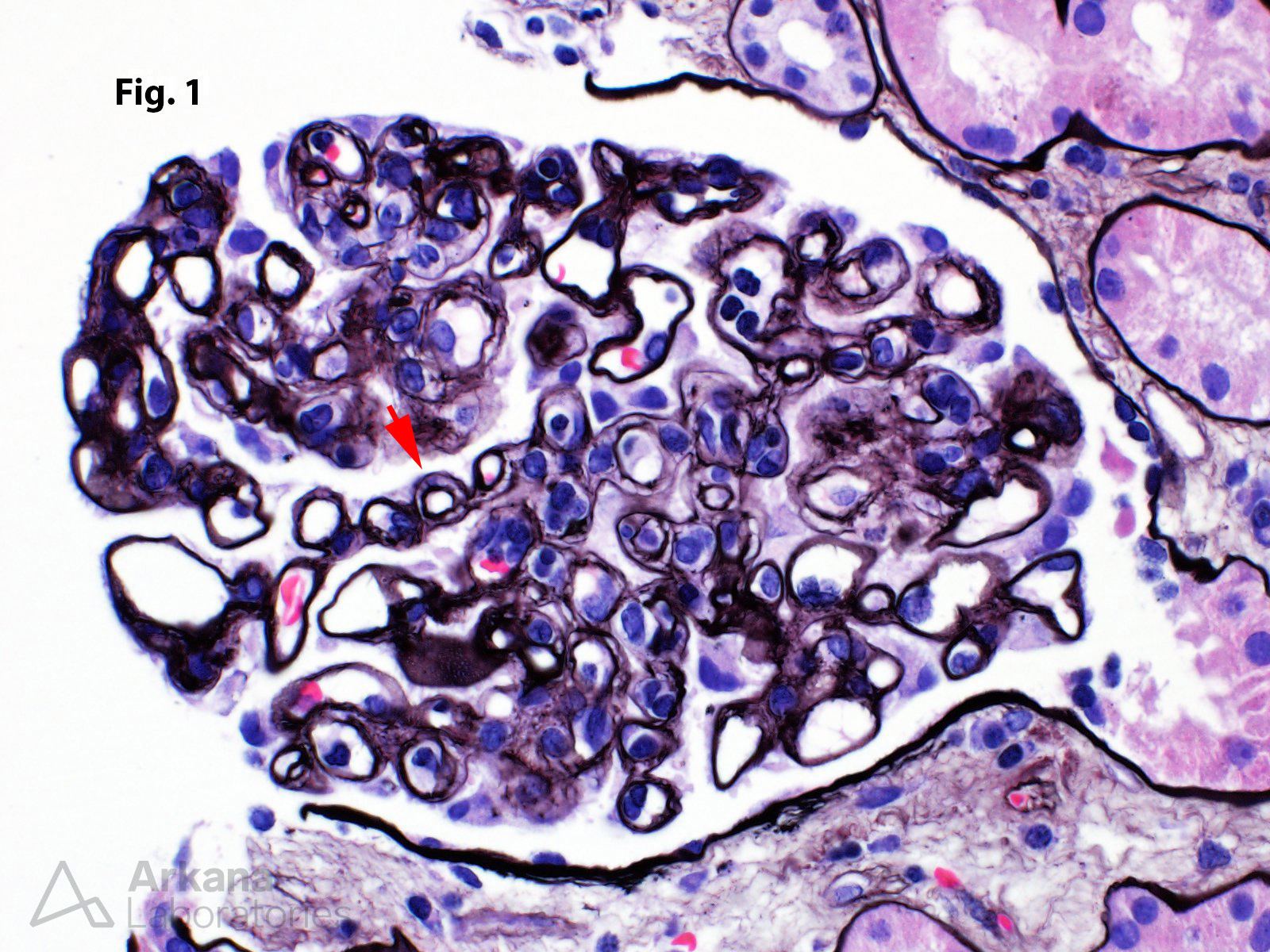
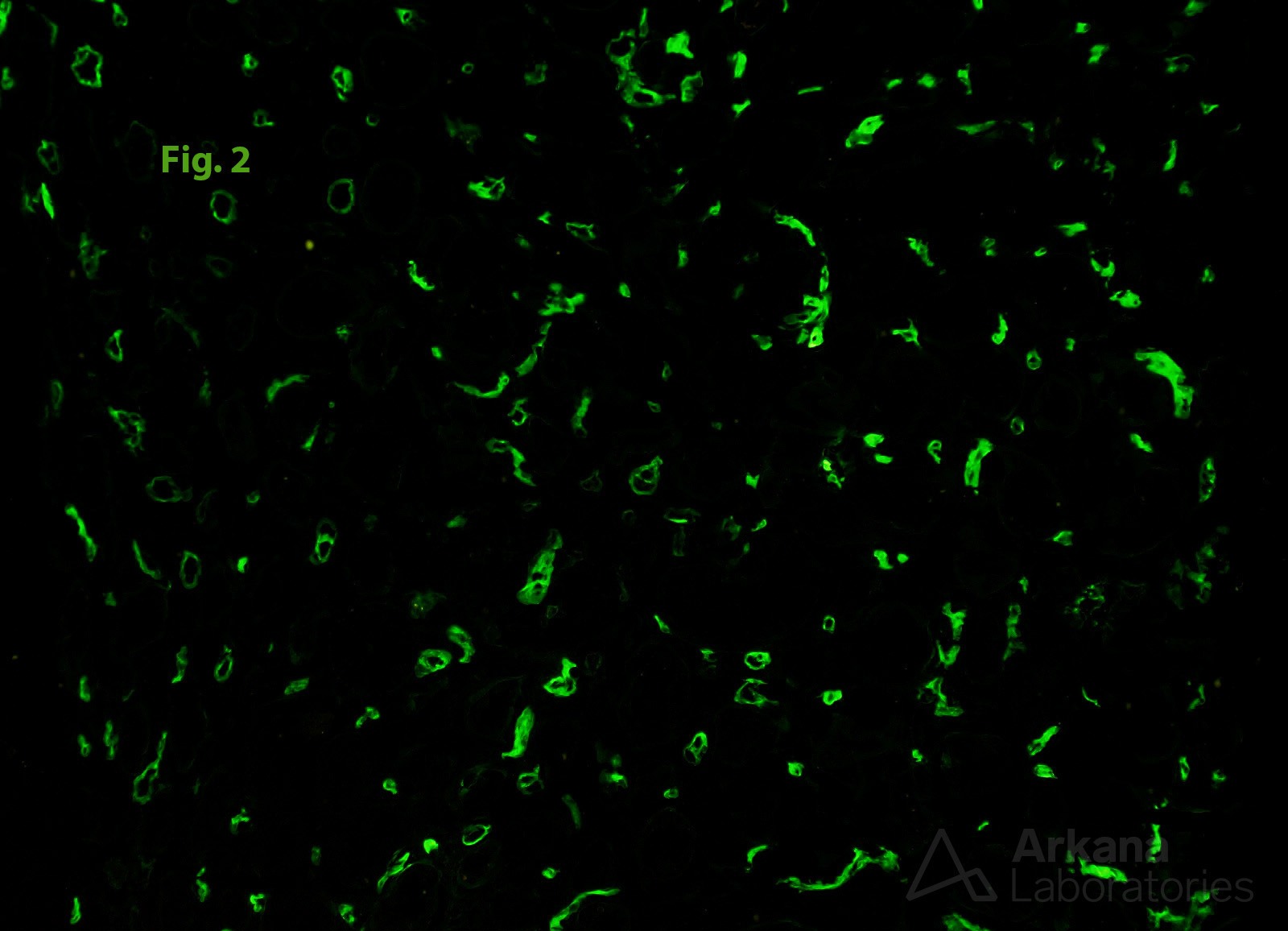
The images are from a patient with an elevated serum creatinine who had undergone living unrelated kidney transplant four years ago. The glomerulus in Figure 1 shows morphologic features of transplant glomerulopathy — the arrow indicates double contour formation involving a capillary loop. Glomerulitis is also present. Figure 2 shows strong and diffuse linear staining of C4d in peritubular capillaries. The findings support a diagnosis of chronic active ABMR.
Reference
Haas M, Loupy A, et al. Am J Transplant. 2018 Feb;18(2):293-307. PubMed PMID: 29243394.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.