
This biopsy came from a 79-year-old patient. He had presented with acute renal failure. His serum creatinine was up to 2.0 mg/dL, from a normal baseline. He also had proteinuria, which was quantified as approximately 1 g. His serum albumin was low at 2.5 g/dL. The patient was anemic, and hemoglobin was 9.1. The patient had been investigated with an extensive serologic work up. ANA was negative, C3 was within normal limits, and SPEP was negative for monoclonal proteins. However, ANCA serologies were positive. Based on that, the patient had been treated with high doses of steroids for a few weeks prior to the biopsy.
The submitted biopsy sample contained one core of renal tissue, mostly from the renal cortex, in which a dozen glomeruli were present. On that sample, one could identify signs of renal disease, or injury, already on low power.
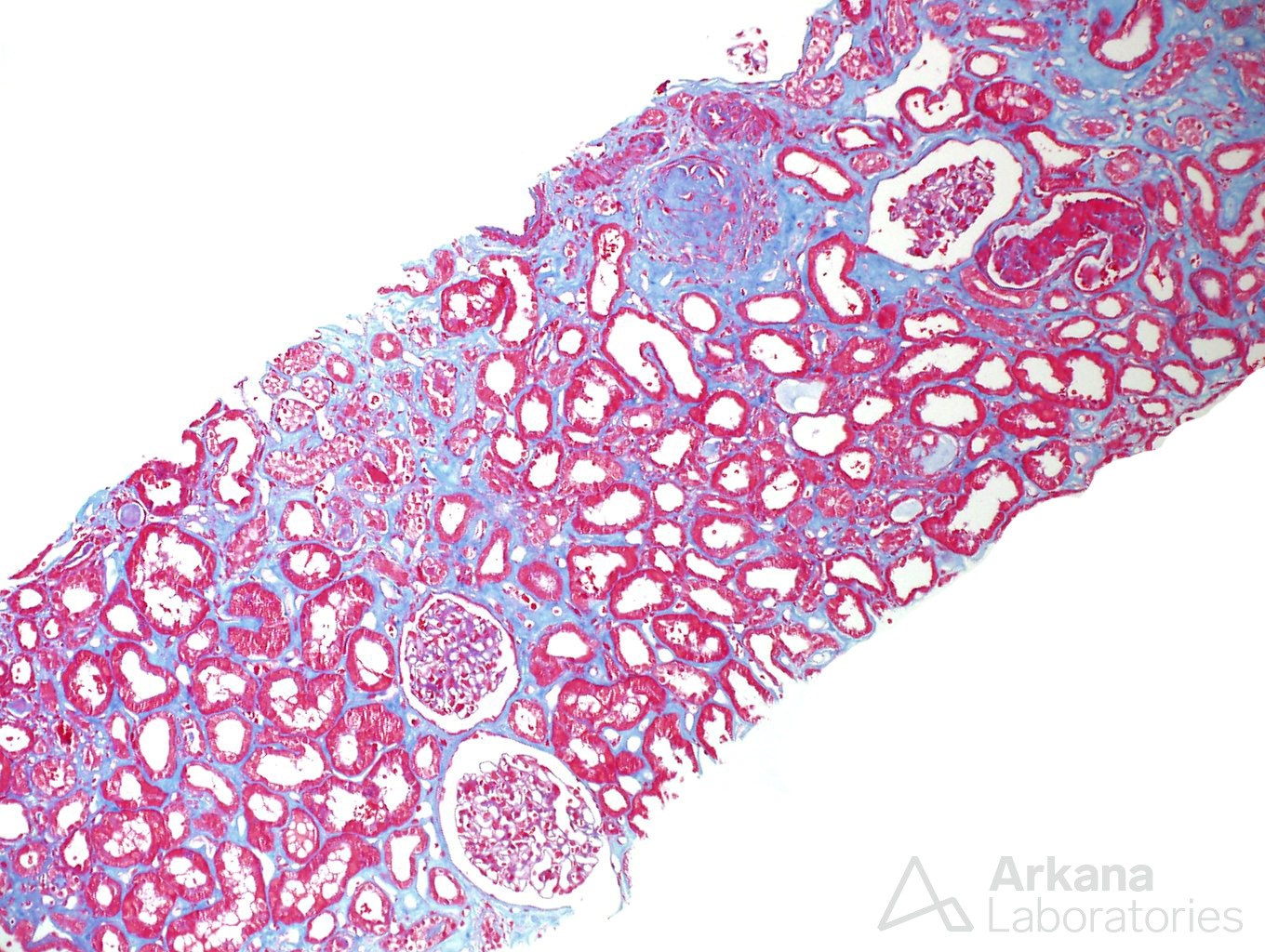
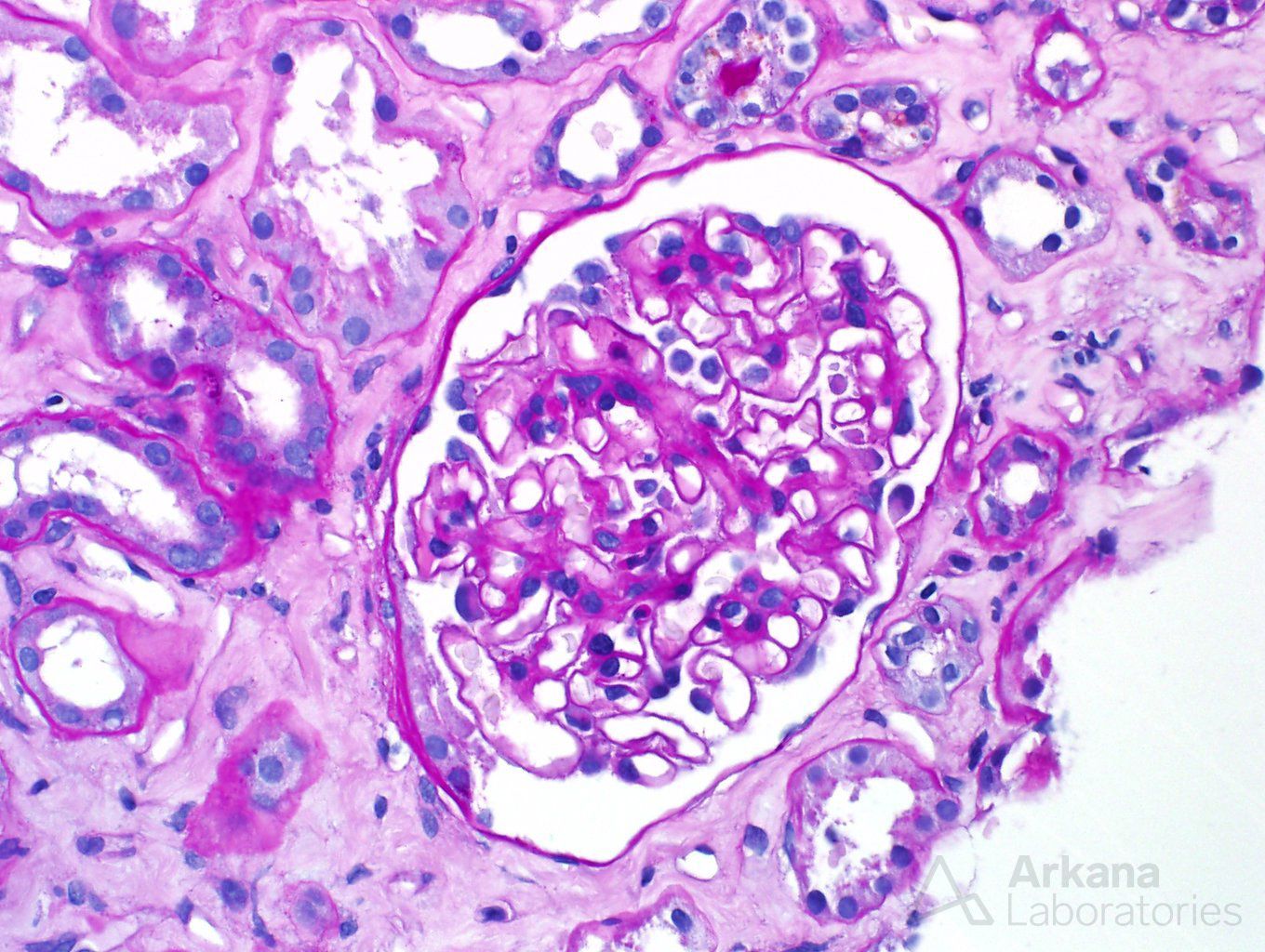
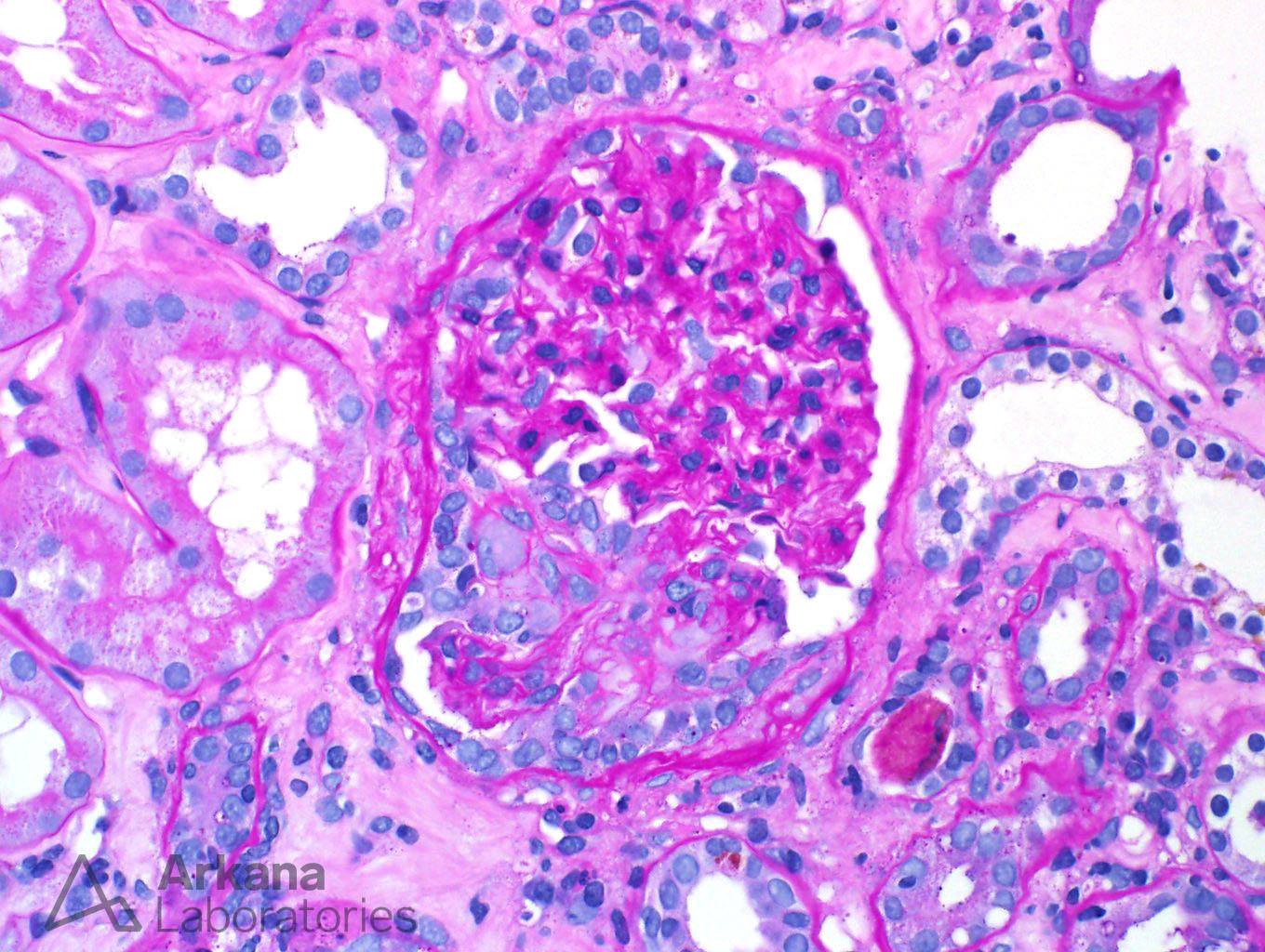
Although most glomeruli had an intact appearance (picture 2), others were clearly abnormal. Areas of atypical segmental glomerulosclerosis were seen, indicating healed areas of glomerular injury, where fibrosis had replaced intact capillary loops (picture 3).
The tubulointerstitial compartment was also carrying harbingers of renal injury. The tubules were dilated and had simplified epithelium – signs of tubular injury. Moreover, some of the tubules had intratubular red blood cells and a few red blood cell casts.
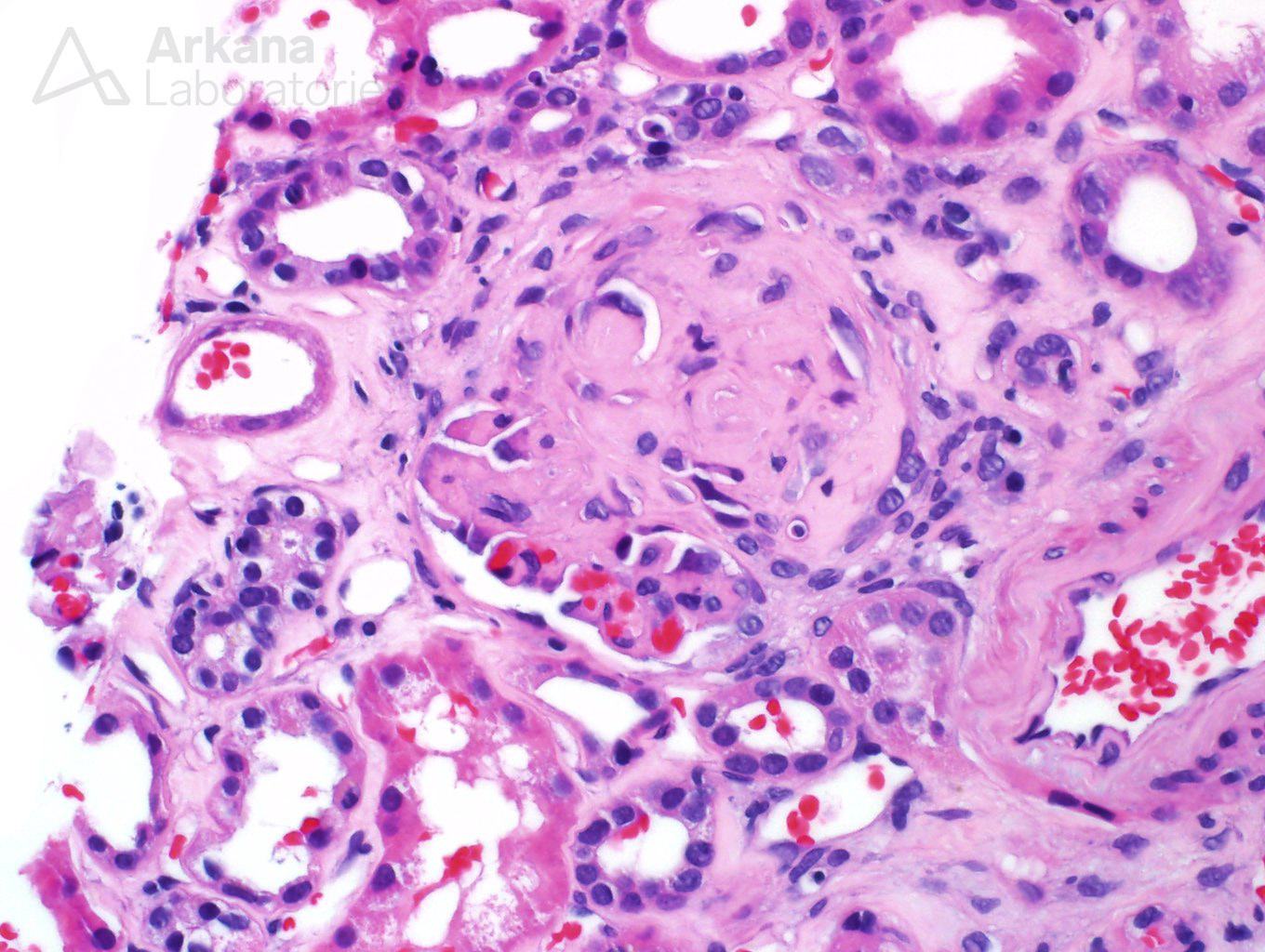
The biopsy was thoroughly examined, following our routine protocol. Sixteen sections of renal tissue were cut, and stained with 6 distinct stains – H&E, PAS, SMMT, Jones Silver stain, trichrome, and Congo red stain- each one with its own characteristics. Yet, despite examination of all the material, no signs of active ANCA disease were present, even though fibrous crescents were identified in some glomeruli (picture 5).
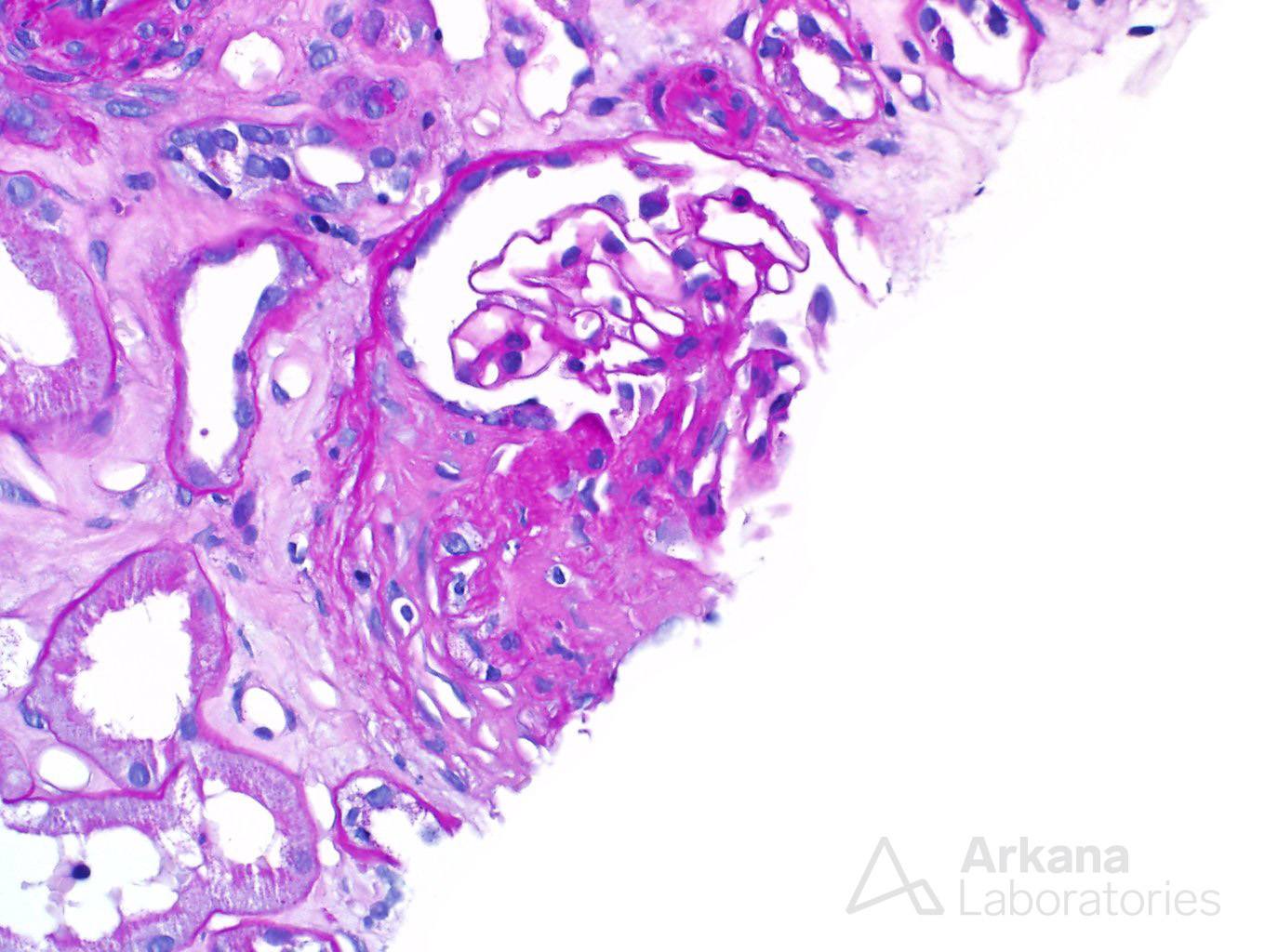
At this point, a diagnosis of sclerosing crescentic glomerulonephritis could have been issued, stating that the biopsy had no signs of activity and showed only chronic changes, as no active cellular crescents or vasculitis were identified.
But, instead of issuing a diagnosis, our physician decided to persist and dig deeper. The triad of red blood cell casts, fibrous crescent, and a very pertinent clinical history, left a taste of unfinished business to the biopsy. Therefore, deeper levels were ordered, literally digging deeper, to look for elusive active glomerular lesions. A total of 6 new slides, 12 sections of tissue, were examined.
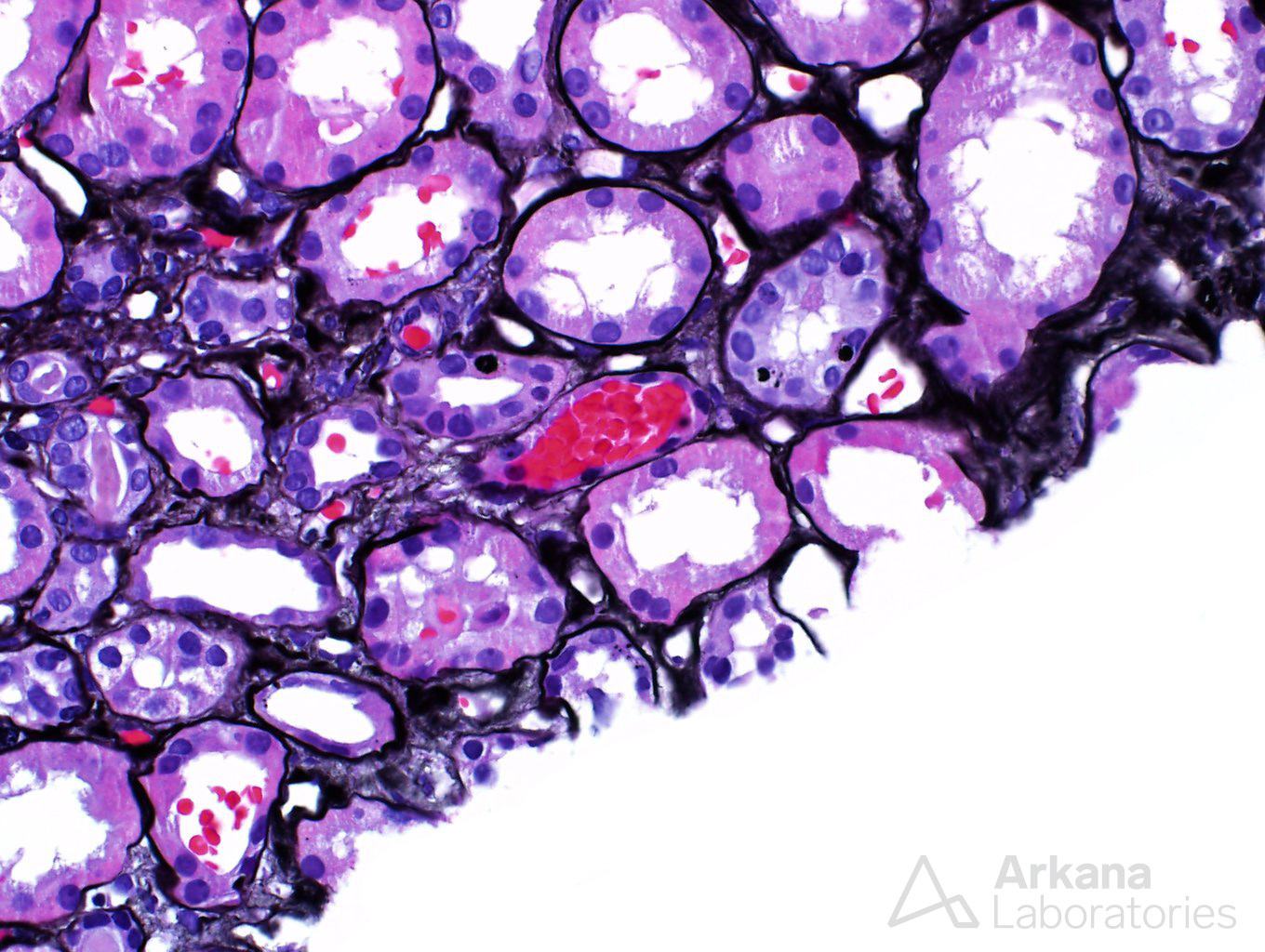
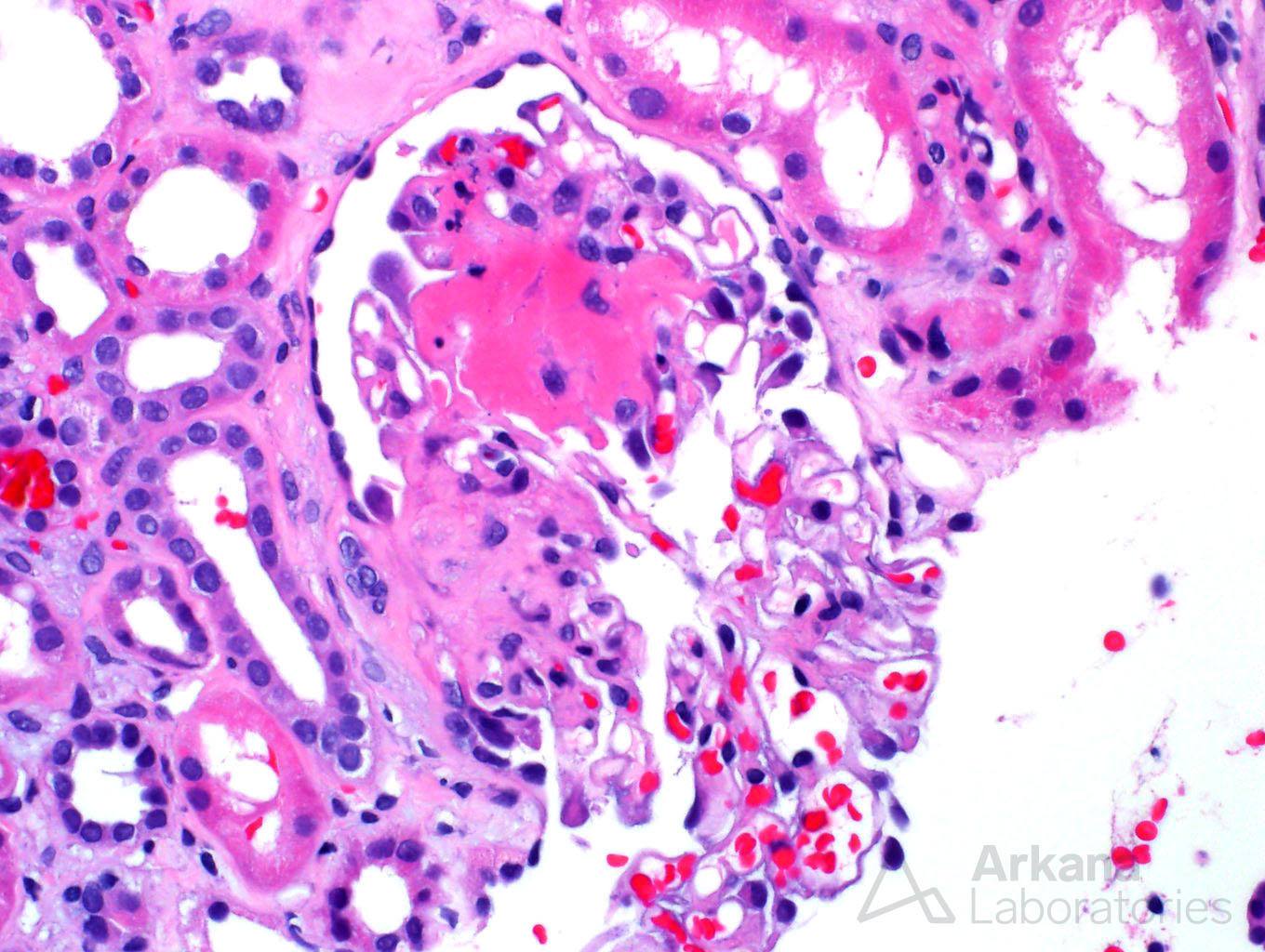
Some say that good things come to those who wait, while others say that good things come to those who hustle. In this case, we did wait and we did hustle, and something came out of it, not necessarily good, but important. In the middle of the deeper sections, we found our elusive, active ANCA disease – a glomerulus with fibrinoid necrosis, and a glomerulus with a cellular crescent (picture 6 and 7).
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.