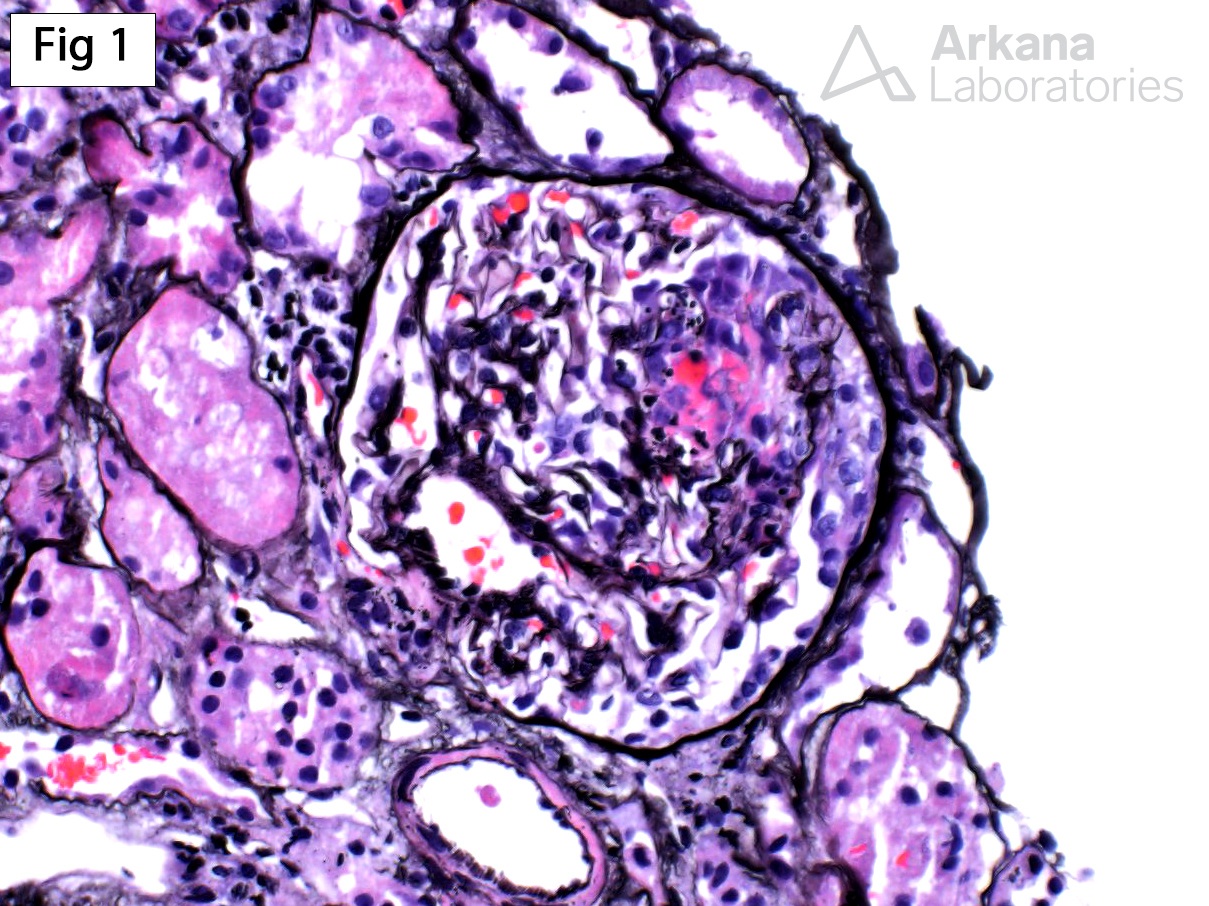
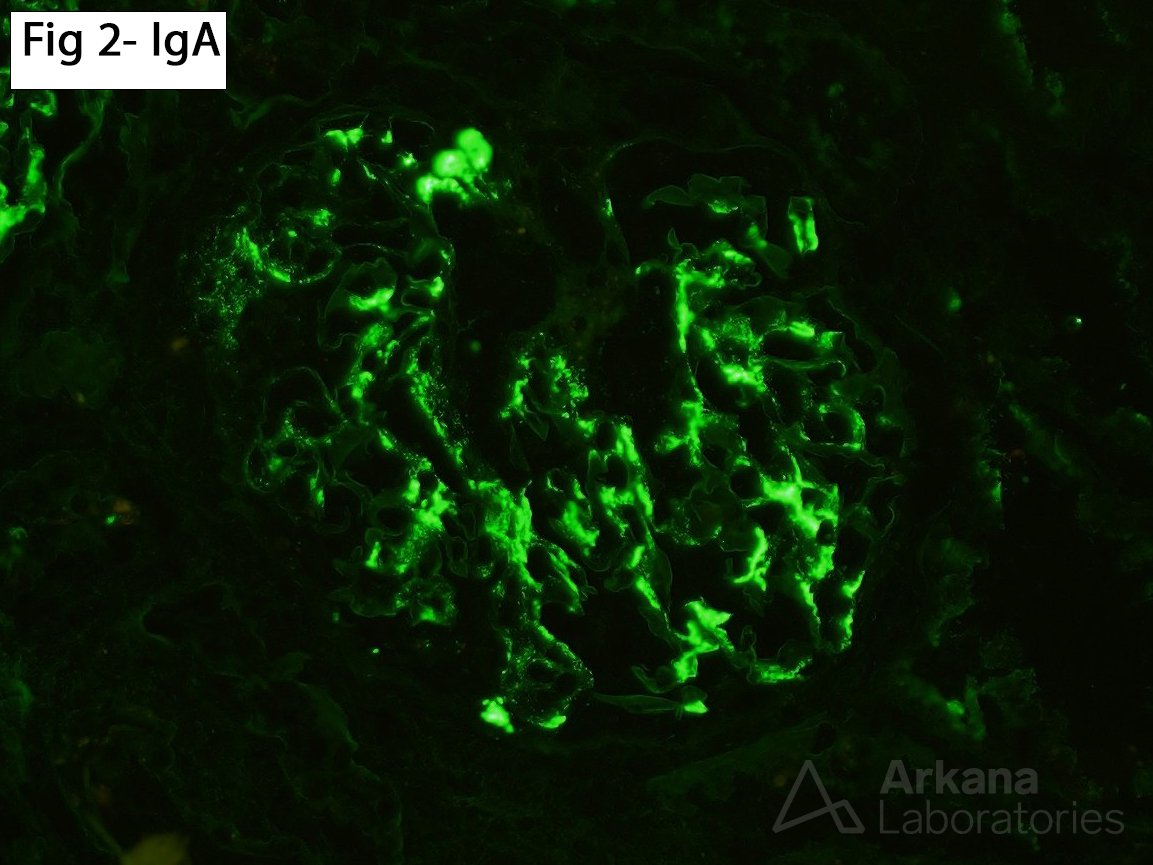
This biopsy was taken from a 58-year-old male with no significant past medical history, who presents with gross hematuria, serum creatinine of 2.5 mg/dl and a urine protein/creatinine ratio of 1.4 g/g. The biopsy shows segmental rupture of the capillary loops associated with fibrinoid necrosis of the glomerular tuft and cellular crescent formation (Fig 1 – Jones stain). Of note, no mesangial or endocapillary proliferation is present. Immunofluorescence (Fig 2) shows mesangial granular staining for IgA (3+), C3 (1+), kappa (2+) and lambda (3+). Electron microscopy (not shown) shows scattered mesangial electron-dense deposits. The differential diagnosis in patients with necrotizing and crescentic glomerulonephritis with IgA deposits includes an IgA-dominant infection-associated glomerulonephritis, a crescentic primary or another secondary form of IgA nephropathy (such as Henoch-Schönlein purpura), and an ANCA-associated glomerulonephritis superimposed on a preexisting/incidental IgA nephropathy. Clinicopathological correlation is essential to reach a definitive diagnosis when this pattern of glomerular injury is encountered.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.