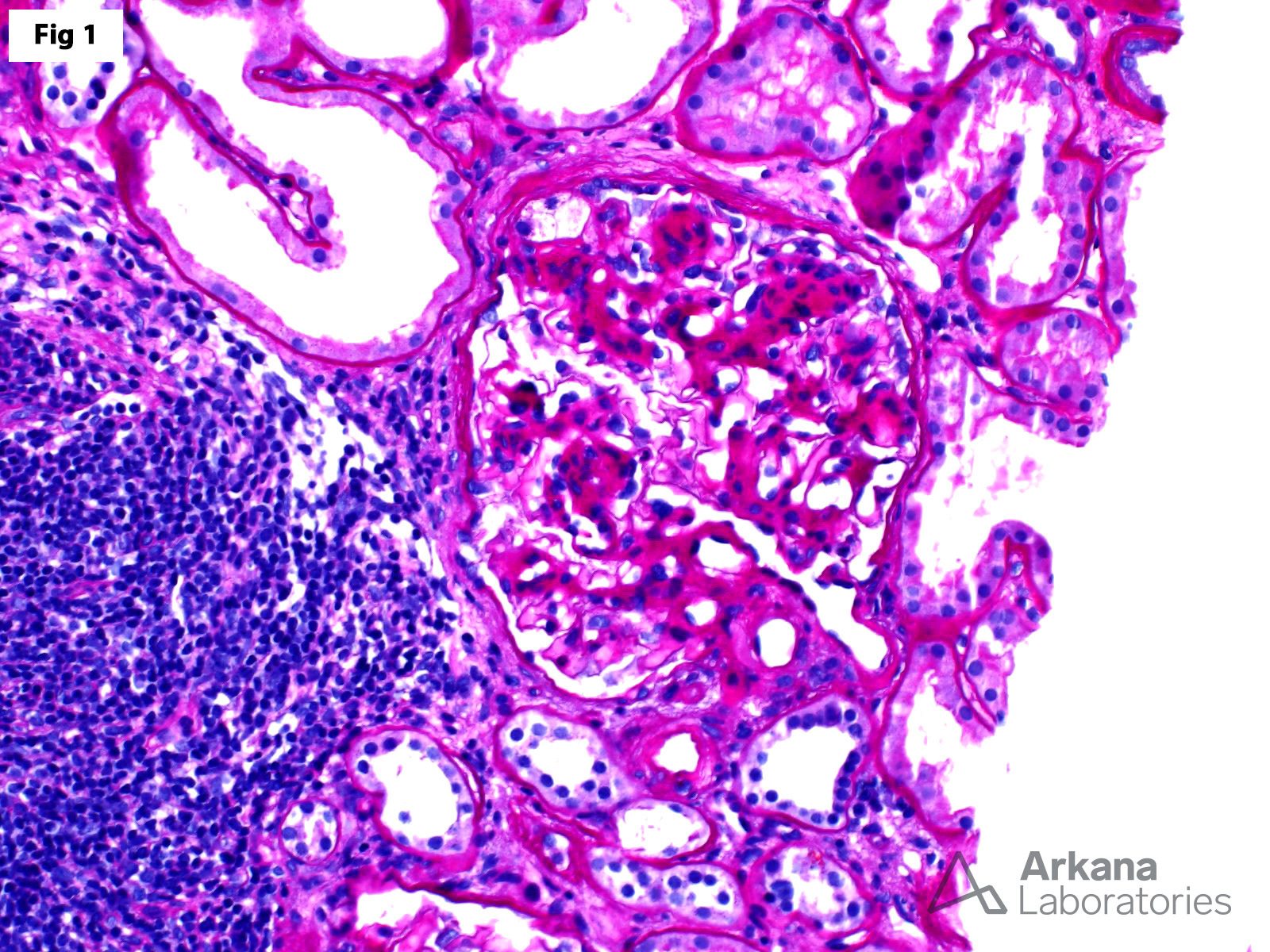
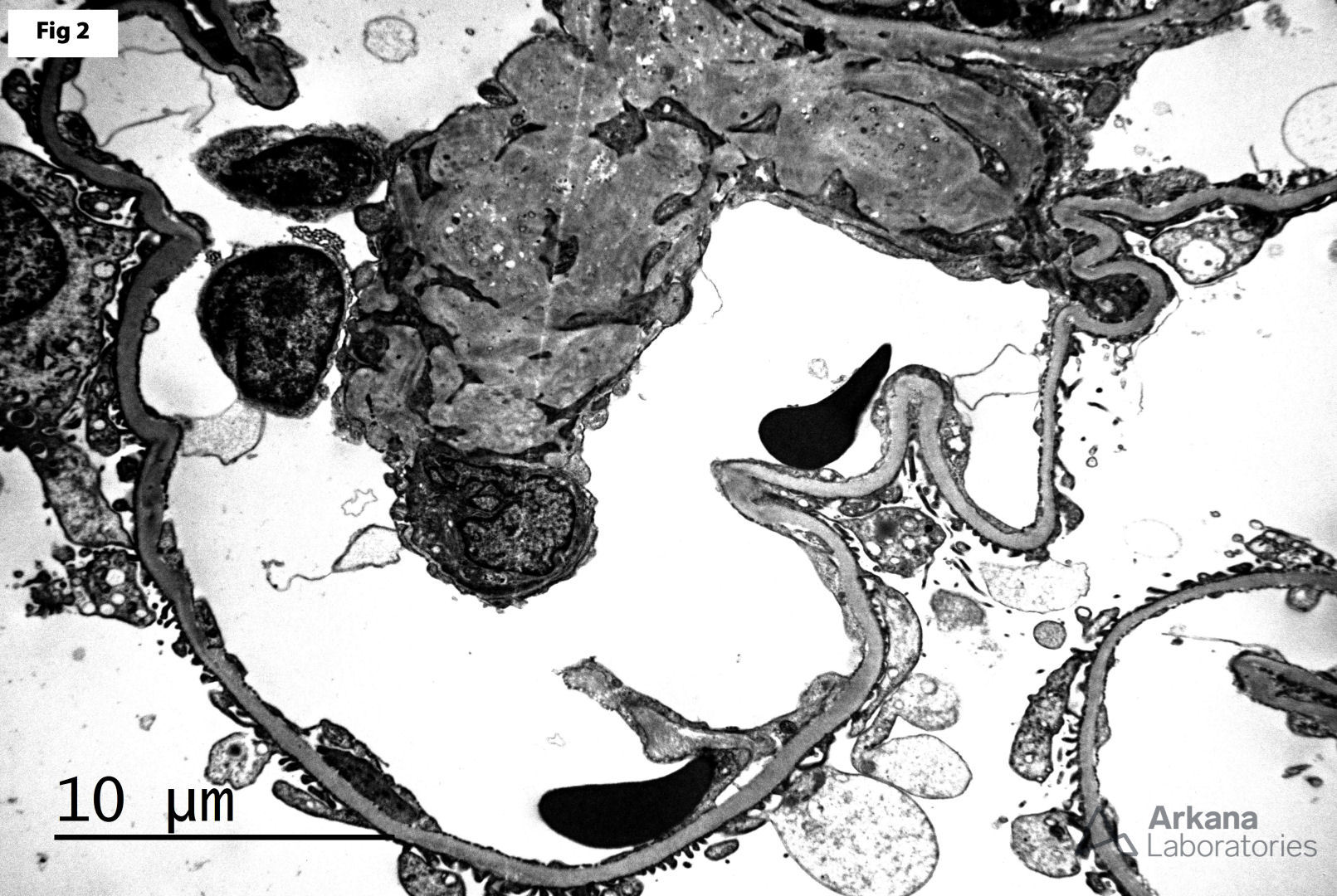
The patient is a 64-year-old male with a history of diabetes mellitus, hypertension, and hyperlipidemia, who presents with an increased creatinine of 1.8 mg/dl and proteinuria (UPCR 2.5 g/g). Serologic workup is completely negative. A renal biopsy was performed and shows nodular glomerulosclerosis (Fig 1) and arteriolar hyalinosis characteristic of diabetic glomerulopathy. Additionally, the glomeruli focally show areas of segmental glomerulosclerosis associated with endocapillary foam cells. These lesions are located at the take-off point of the proximal tubule (Fig 1) and reminiscent of the glomerular lesions seen in the tip variant of FSGS. Electron microscopy shows mesangial matrix expansion, mostly intact epithelial foot processes and absence of electron dense deposits (Fig 2). While FSGS tip variant most commonly represents a primary podocytopathy (primary FSGS), similar lesions may be seen in other glomerulopathies with heavy proteinuria, including diabetic glomerulopathy and membranous glomerulopathy, among others. The absence of significant epithelial foot process effacement in this case, along with the presence of changes characteristic of diabetic glomerulopathy in the setting of subnephrotic proteinuria, significantly decreases the likelihood a primary podocytopathy.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.