Monday
Onco-nephrology is a rapidly developing area of nephrology designed to help address and prevent kidney problems and the many complex issues that arise in cancer patients.
AKI is a common complication in cancer patients. The highest 1-year risk of AKI was seen in patients with kidney cancer (44%), liver cancer (33%), and multiple myeloma (31.8%) in one large population-based cohort study. Patients with distant metastases were at highest risk. https://www.ncbi.nlm.nih.gov/pubmed/21767759
What is the most common glomerular pathology reported in patients with solid tumors?
- Minimal change disease
- Membranoproliferative glomerulonephritis
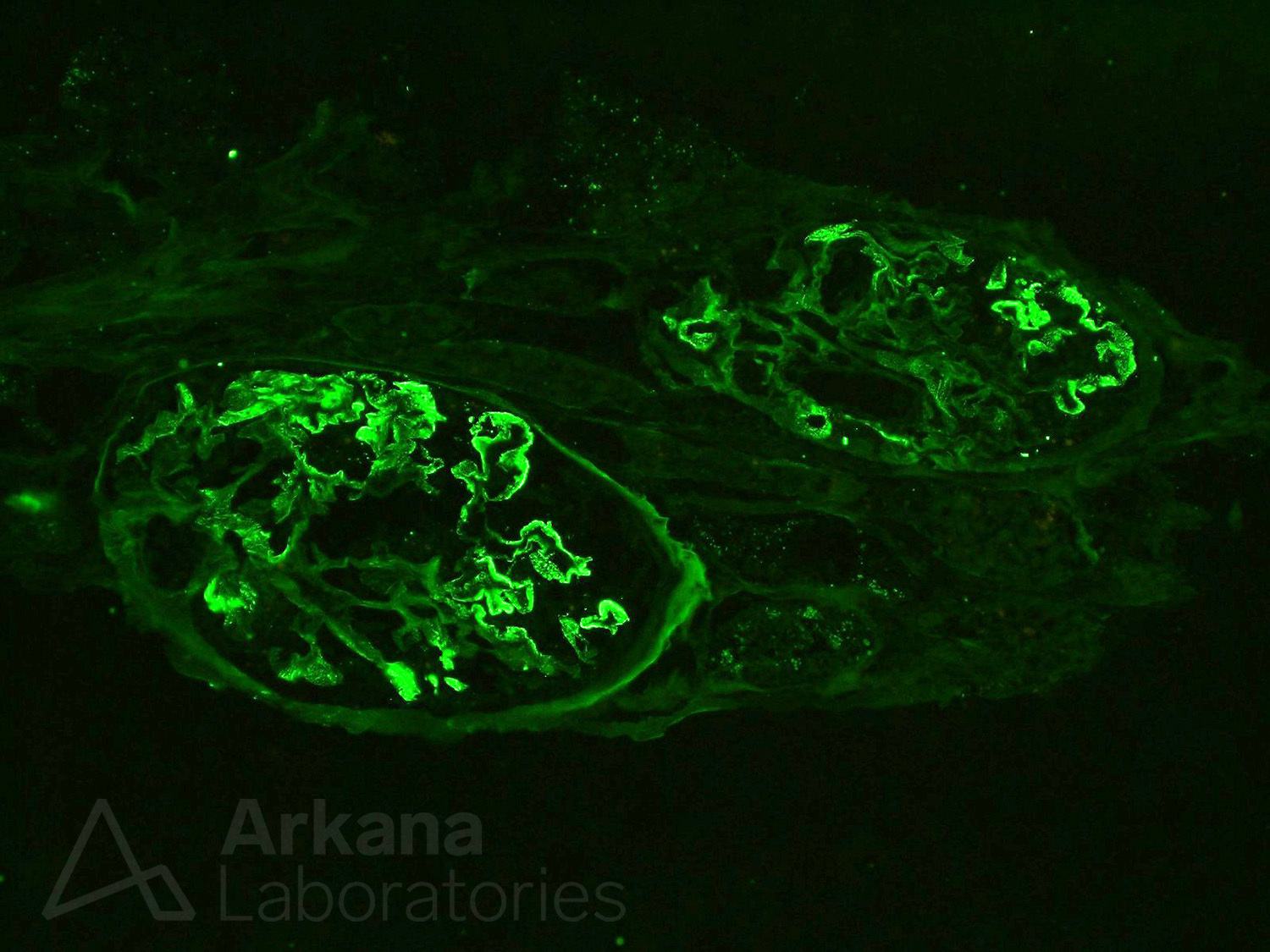
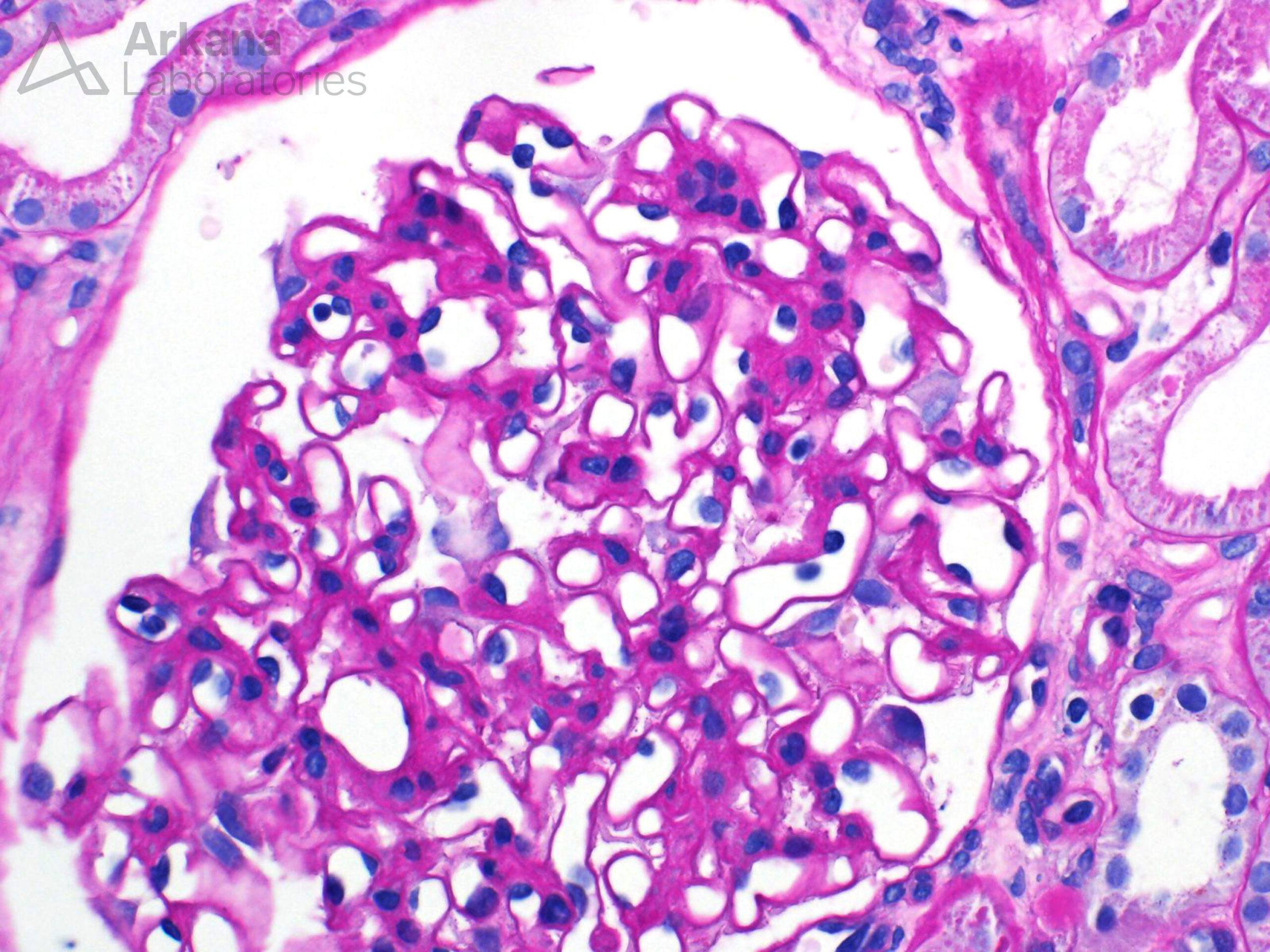
- Membranous nephropathy
- Thrombotic microangiopathy
Answer: Membranous nephropathy. The incidence of cancer was significantly higher in patients with MN than in the general population (standardized incidence ratio 9.8 [5.5-16.2] for men and 12.3 [4.5-26.9] for women). https://www.ncbi.nlm.nih.gov/pubmed/16941021
In patients with cancer-associated membranous nephropathy, there was a strong relationship between reduction of proteinuria and clinical remission of cancer (P < 0.001). https://www.ncbi.nlm.nih.gov/pubmed/16941021
Although there are case reports of THSD7A-associated membranous nephropathy and cancer, the largest case series published by Arkana showed only 2 of the 31 patients had a history of cancer and none were diagnosed with malignancy on follow-up. https://www.ncbi.nlm.nih.gov/pubmed/29243738
Tuesday
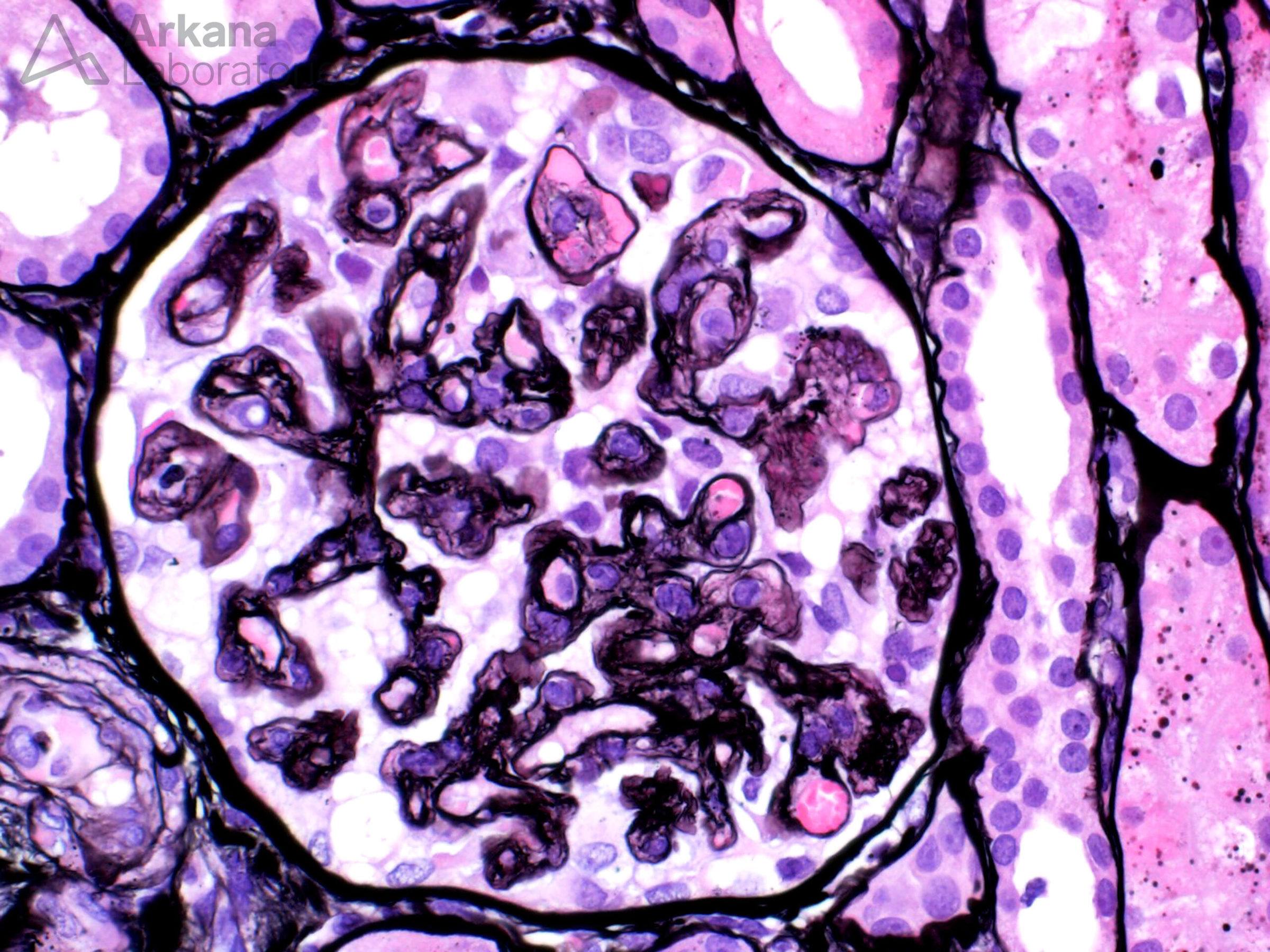
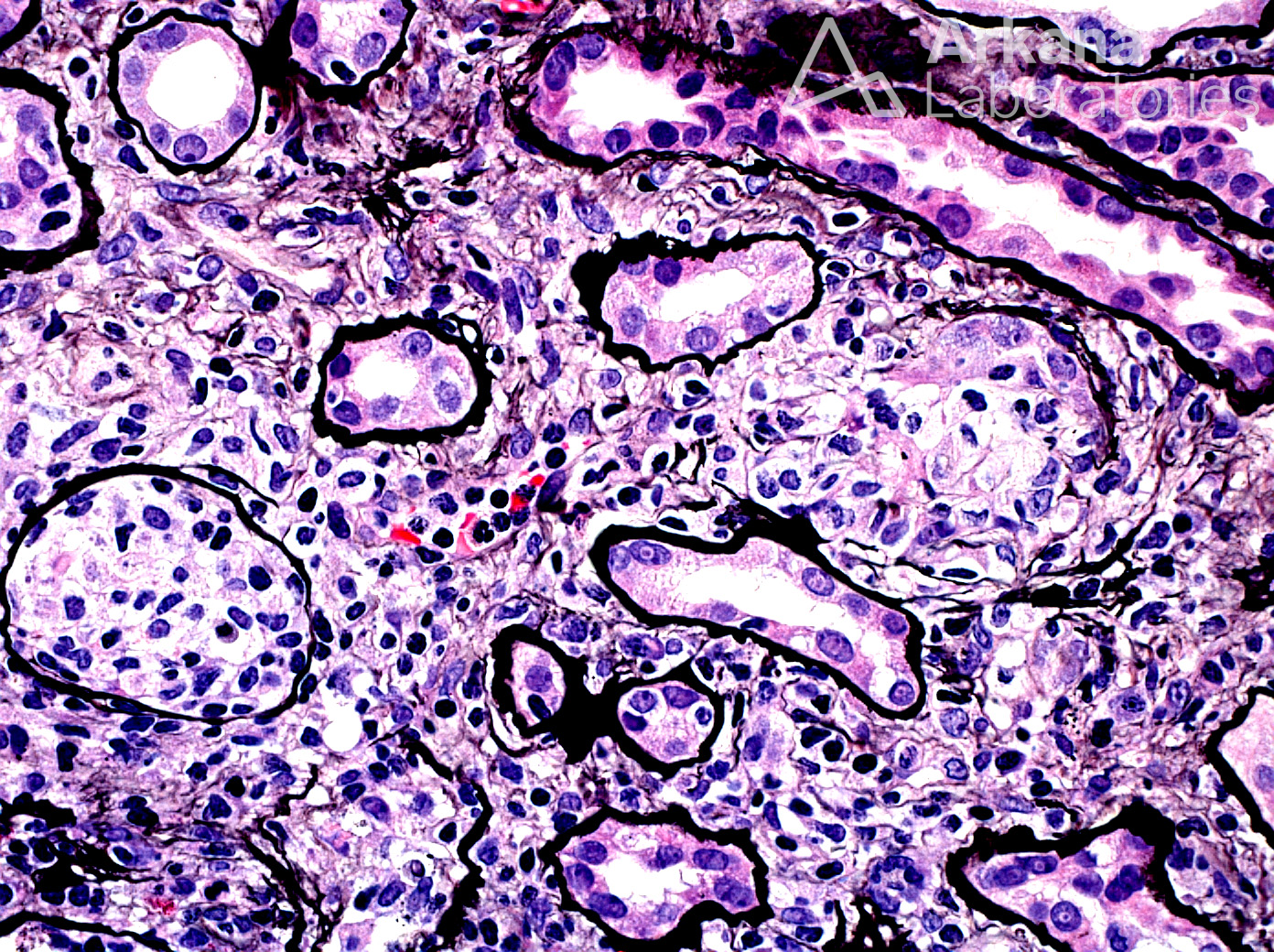
Myeloproliferative neoplasm-related glomerulopathy is most commonly seen in the setting of primary myelofibrosis and is characterized by variable degrees of mesangial sclerosis & hypercellularity, segmental sclerosis, and occasionally features of chronic thrombotic microangiopathy. https://www.ncbi.nlm.nih.gov/pubmed/21654720
Lysozyme-induced kidney disease is characterized by proteinuria and progressive decrease in kidney function. It is most commonly seen in the setting of chronic myelomonocytic leukemia (CMML). In newly diagnosed CMML patients, plasma lysozyme levels are positively correlated with both absolute monocyte count and serum creatinine.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2724597/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6553339/
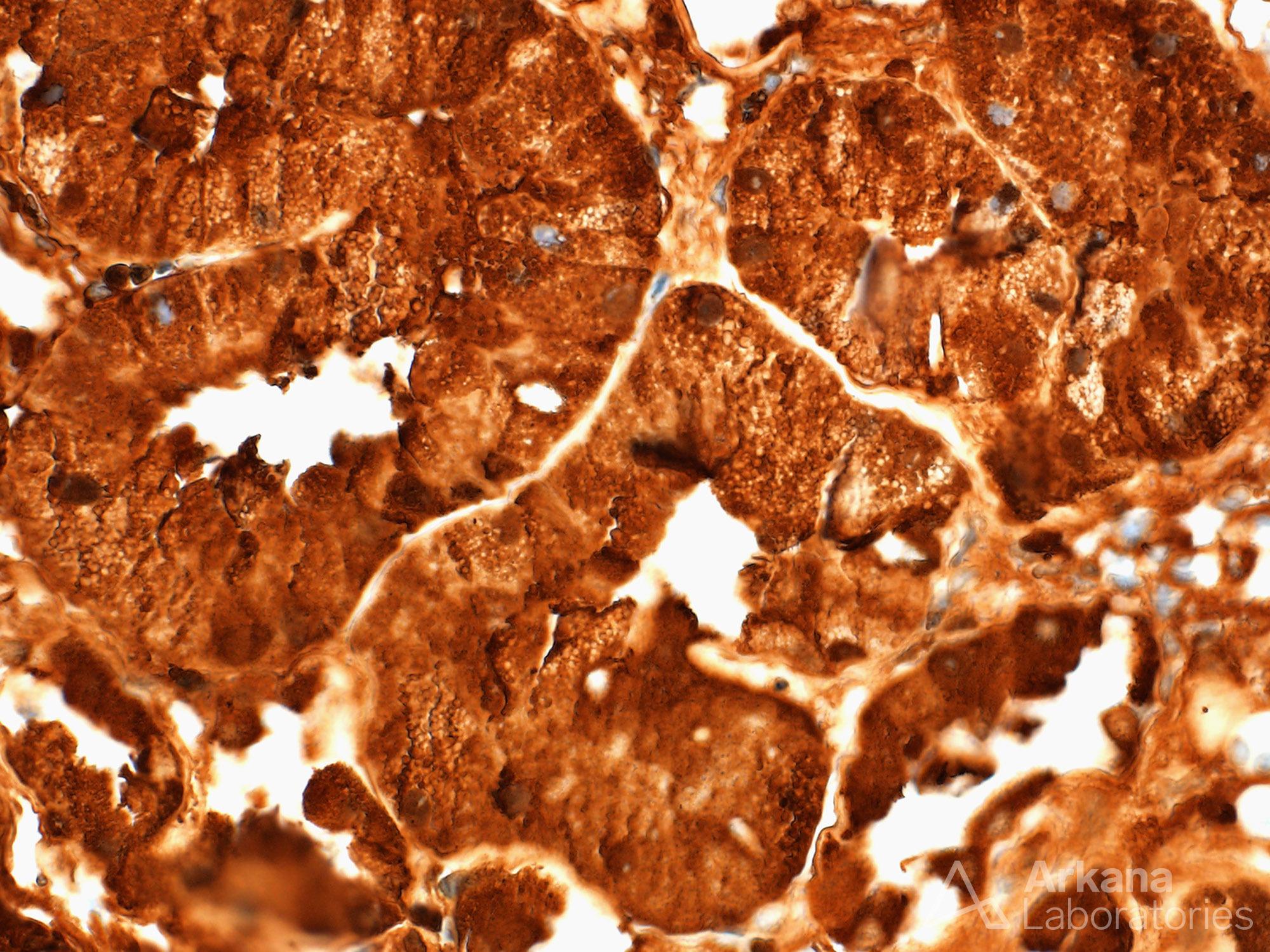
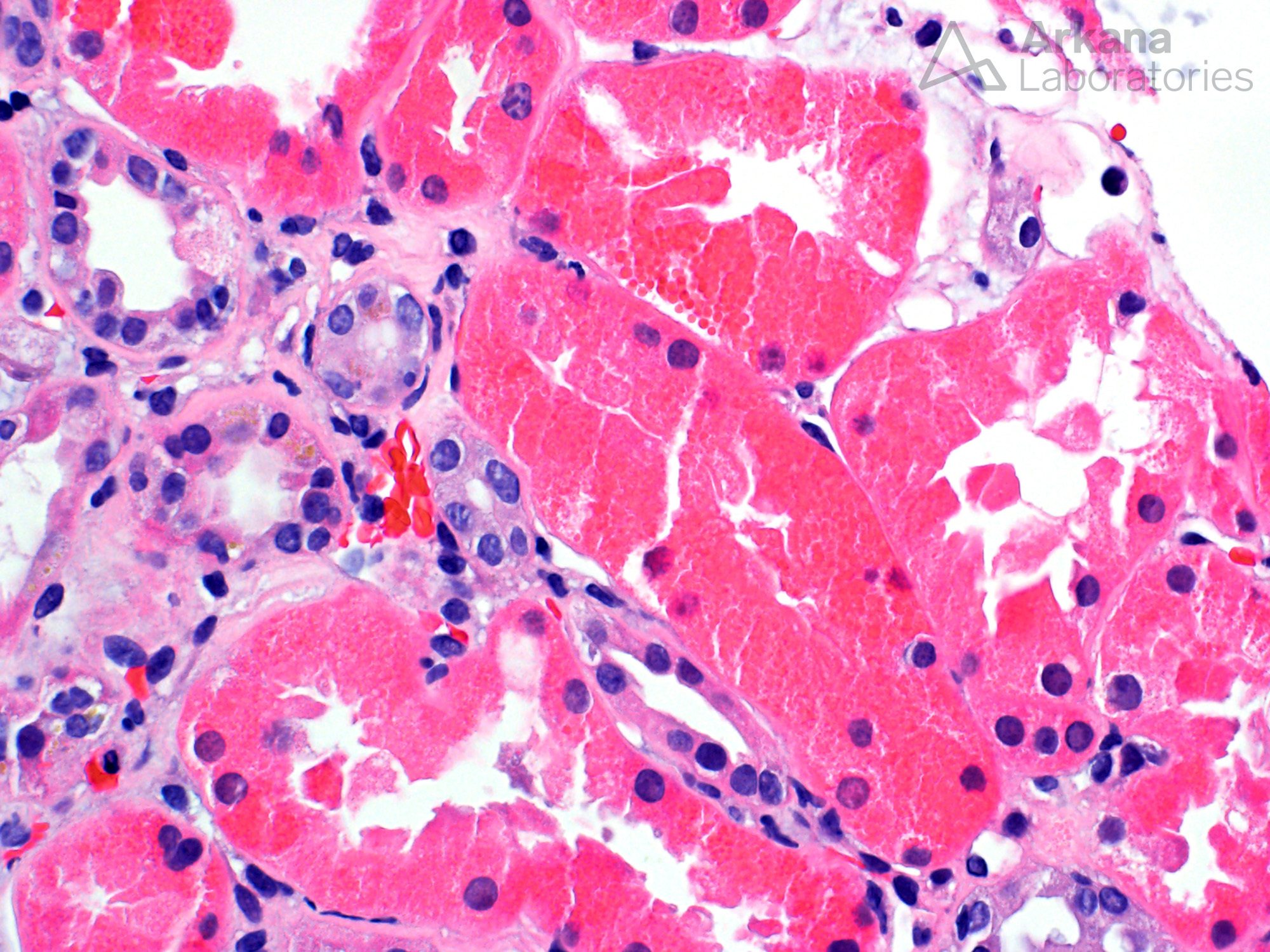
In newly diagnosed CMML patients, plasma lysozyme levels are positively correlated with both absolute monocyte count and serum creatinine.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2724597/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6553339/
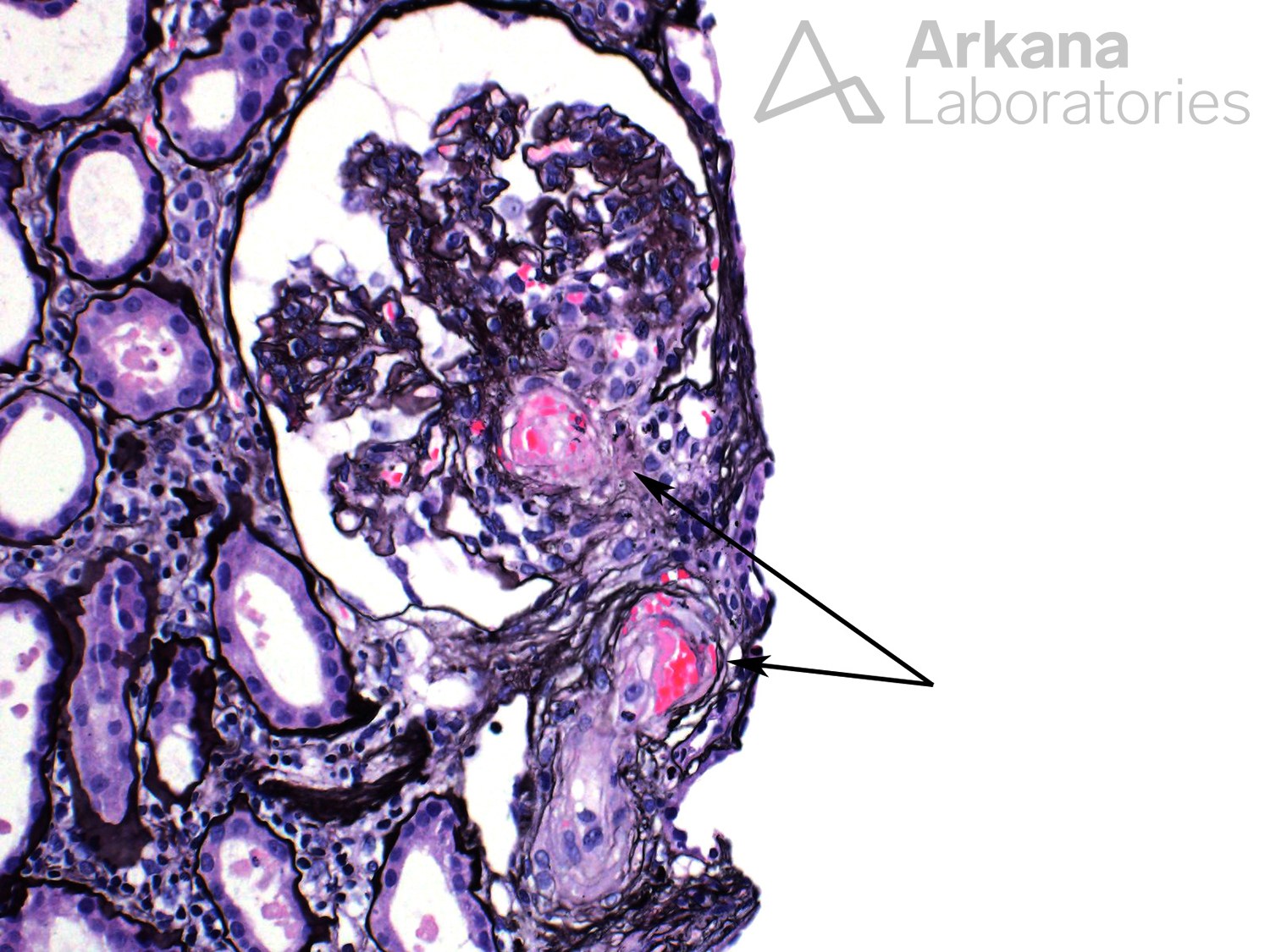
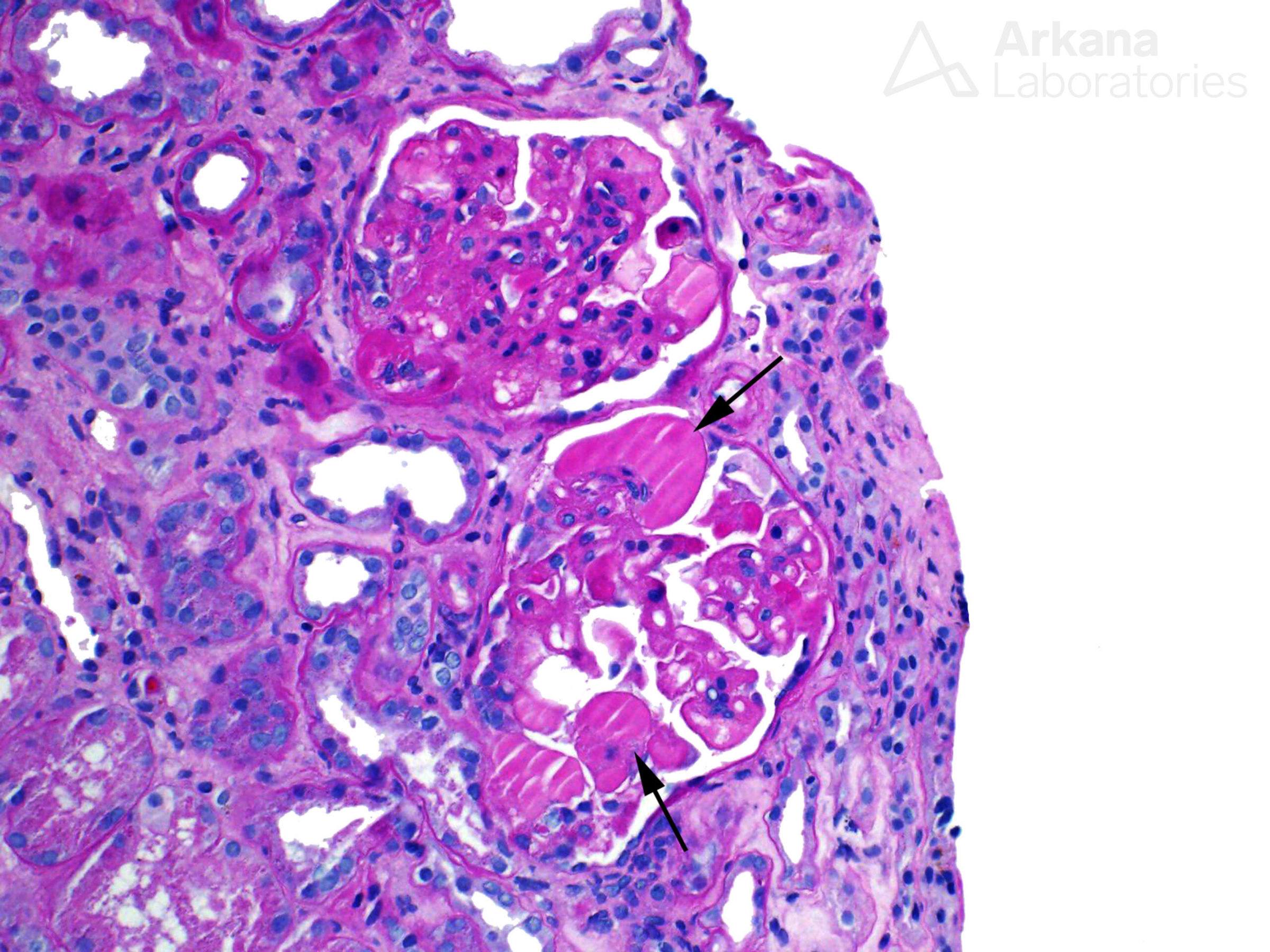
Most cases of cancer-associated TMA have been reported in patients with mucin producing adenocarcinomas, predominantly gastric, breast, lung, and prostate. A majority of patients have metastatic disease. Plasma exchange is rarely effective but response to chemotherapy is often achieved.
https://www.ncbi.nlm.nih.gov/pubmed/17034030
https://www.ncbi.nlm.nih.gov/pubmed/22732949
A majority of patients with cancer-associated TMA have metastatic disease. Plasma exchange is rarely effective but response to chemotherapy is often achieved.
https://www.ncbi.nlm.nih.gov/pubmed/17034030
https://www.ncbi.nlm.nih.gov/pubmed/22732949
TMA has also been associated with monoclonal gammopathy and C3 glomerulopathy via paraprotein-related dysregulation of the alternative complement pathway.
https://journals.sagepub.com/doi/full/10.1177/2399369318822593
Wednesday
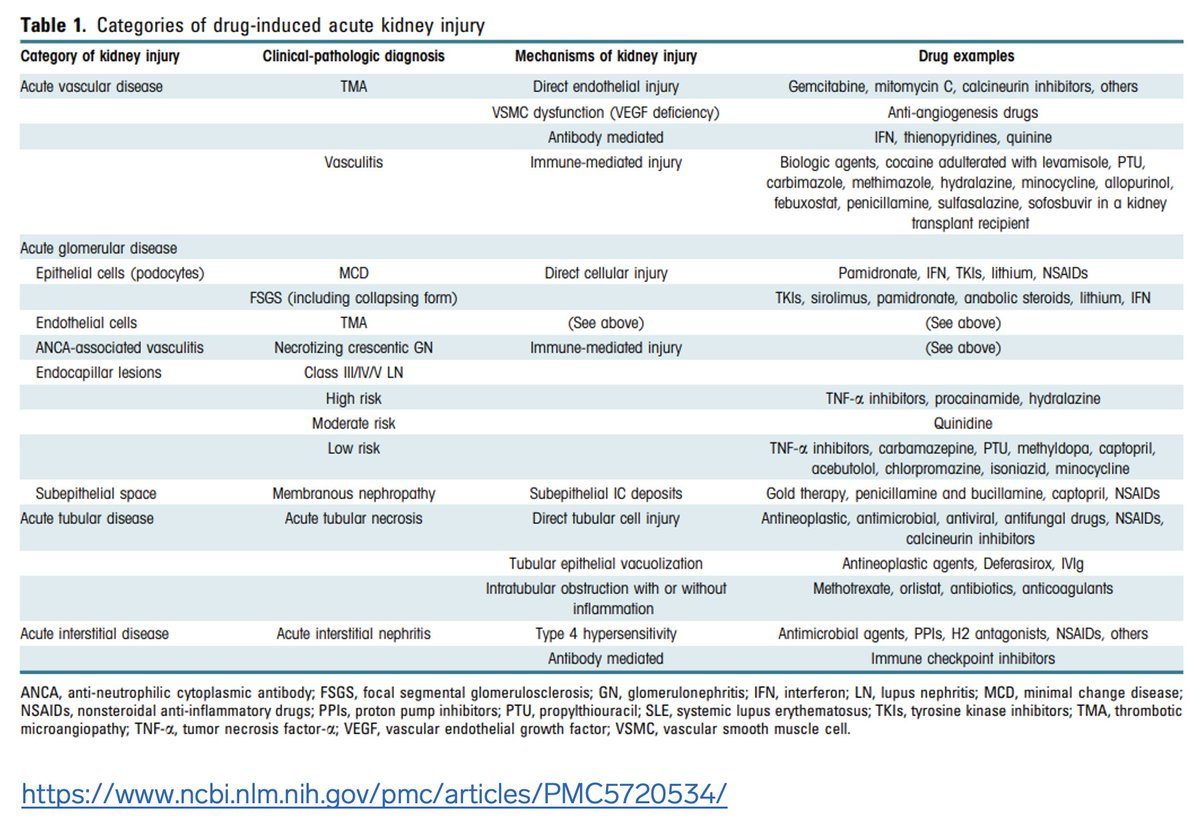
There are many risk factors for chemotherapy-induced nephrotoxicity beyond innate drug toxicity to include patient factors (such as older age and pharmacogenetics), tumor-related kidney effects (direct and indirect), and kidney drug handling. https://www.ncbi.nlm.nih.gov/pubmed/22879440
Gemcitabine-related AKI usually manifests as thrombotic microangiopathy (TMA) and often presents with new-onset or worsening hypertension in addition to MAHA and thrombocytopenia. Onset of TMA is often delayed with a mean time ranging from 6-10 months after initiation of therapy. https://www.ncbi.nlm.nih.gov/pubmed/19203505
Literature reviews of gemcitabine-related TMA show no difference in outcomes between pts treated with plasmapheresis and conservative management with drug withdrawal.
https://www.ncbi.nlm.nih.gov/pubmed/19816959
Eculizumab has also been used in gemcitabine-related TMA with mixed response rates when compared to supportive care alone.
https://www.ncbi.nlm.nih.gov/pubmed/29329518
https://www.ncbi.nlm.nih.gov/pubmed/24490050
TMA is the predominant glomerular lesion associated with anti-VEGF therapy. It has been reported after IV and intraocular use. It has prominent hyaline-like thrombi that can be confused for cryoglobulinemic GN.
ttps://www.ncbi.nlm.nih.gov/pubmed/18337603
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4602430/
Thursday
There are now several currently available immune checkpoint inhibitors with increasing indications for both solid tumor and hematologic malignancies.
https://www.ncbi.nlm.nih.gov/pubmed/31303350
New inhibitory checkpoints and their target molecules are continually being investigated to expand the use and efficacy of existing immune checkpoint inhibition therapy.
https://jhoonline.biomedcentral.com/articles/10.1186/s13045-021-01056-8
https://jhoonline.biomedcentral.com/articles/10.1186/s13045-021-01056-8/tables/1
Side effects of immune checkpoint inhibitors are often related to off-target inflammatory responses that can affect almost every organ system. Their manifestations can closely resemble autoimmune diseases.
https://www.ncbi.nlm.nih.gov/pubmed/31303350
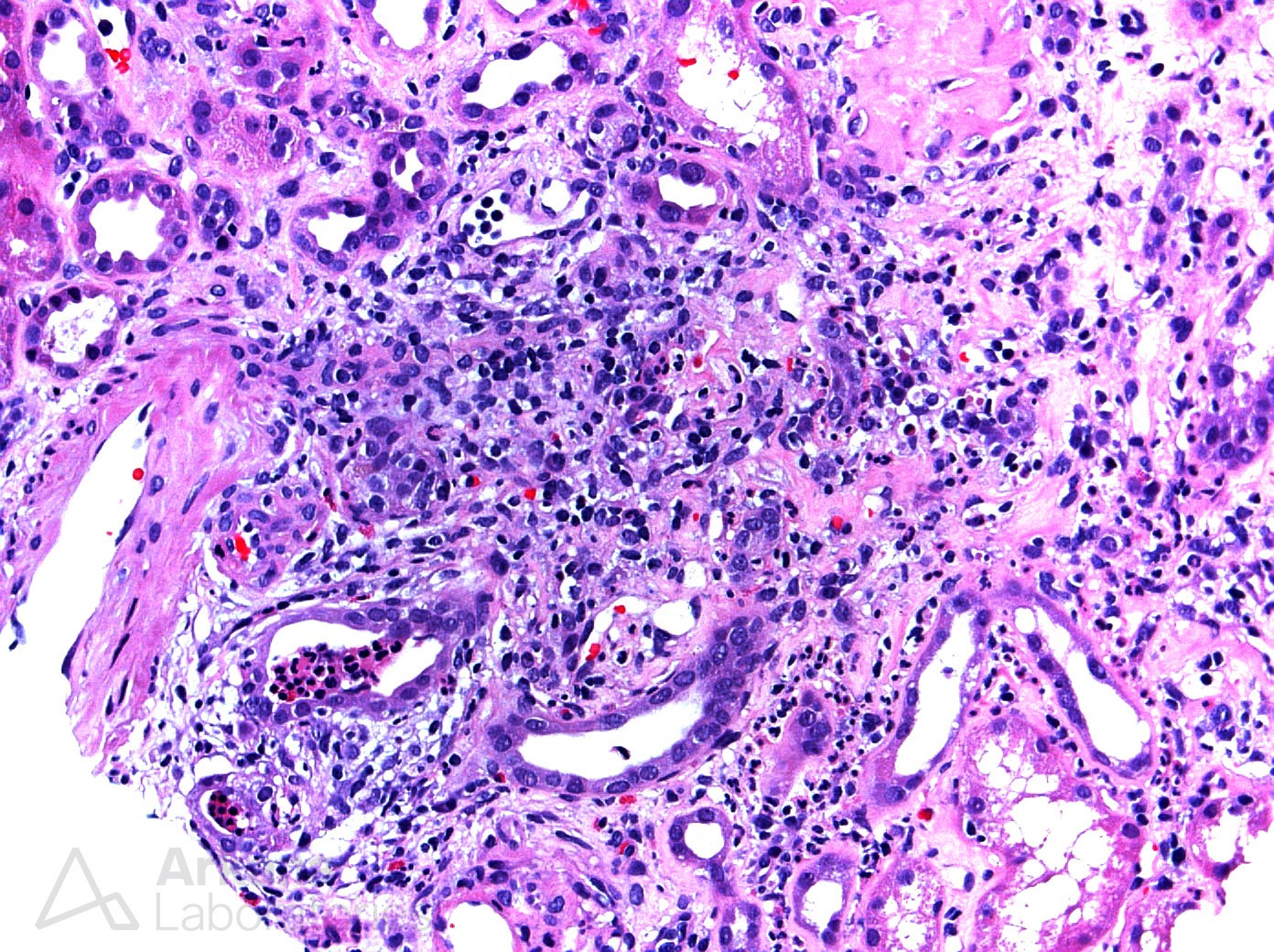
The most common finding on kidney biopsy in patients with checkpoint inhibitor–induced AKI is acute tubulointerstitial nephritis. Oral glucocorticoids are typically given for symptoms persisting more than 1 week after drug withheld.
https://www.ncbi.nlm.nih.gov/pubmed/27282937
Cases of acute cellular rejection have also been reported in patients on checkpoint inhibitors in the kidney allograft.
https://www.ncbi.nlm.nih.gov/pubmed/26988410
Hematopoietic cell transplantation-related kidney injury is often multifactorial to include such factors as chemo/radiation, infection, immunosuppressive agents, recurrence/persistence of original disease, and GVHD.
https://www.ncbi.nlm.nih.gov/pubmed/17702721
https://www.ncbi.nlm.nih.gov/pubmed/27015134
The most common glomerular lesion on kidney biopsy in hematopoietic cell transplantation pts is membranous nephropathy. It’s often seen with clinical evidence of chronic GVHD. Minimal change disease, TMA, acute tubular injury, amyloidosis, and polyomavirus can also be seen.

Friday
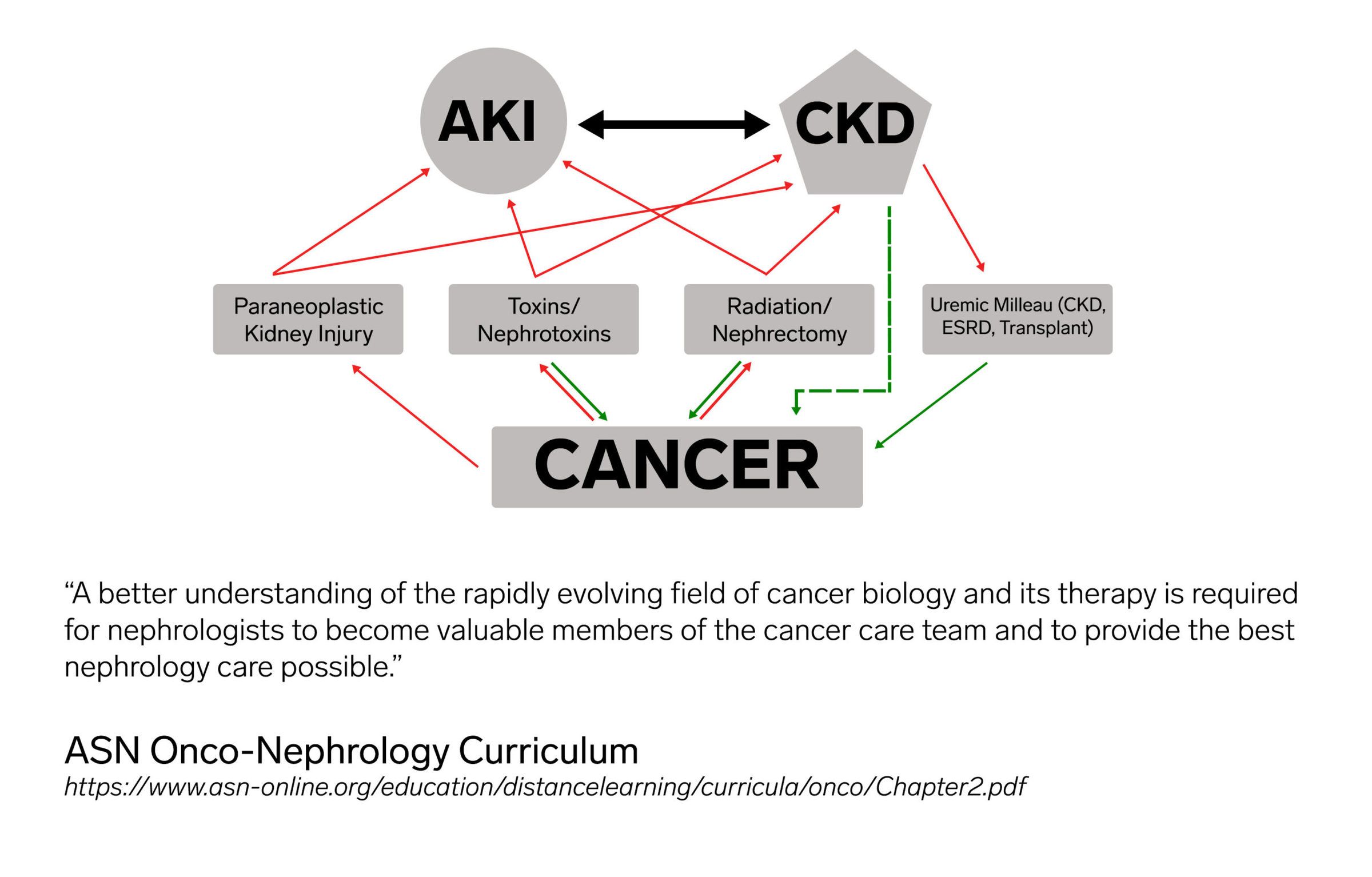
The rapidly evolving field of oncology and cancer management creates unique opportunities as well as challenges for the nephrology community. As such, it is important for nephrologists and nephropathologists to be informed and involved in its many aspects in order to better care for patients and be valuable members of a multidisciplinary cancer care team. The renal manifestations and complications of cancer are myriad and include acute as well as chronic kidney injury, electrolyte/acid–base disturbances, direct injury of the kidney through tumor infiltration and/or paraneoplastic substances, pharmacokinetics of chemotherapeutic agents, and hematopoietic cell transplantation-related kidney injury. Kidney transplant patients also have an increased risk of cancer, which is often more aggressive, making routine surveillance and early detection and treatment essential. As nephropathologists, we have seen increasing biopsies with acute and chronic kidney injury related to newer chemotherapies and immunotherapies as well as effects of stem cell transplantation. Finally, the importance of early palliative care for patients with advanced kidney disease and cancer should not be overlooked as well as the possibility of incorporating palliative care into dialysis facility patient care. I hope I have convinced you this week that the field of onco-nephrology is continually advancing and vitally important as we care for an increasing number of cancer patients in our practices. Luckily, the ASN has a comprehensive online curriculum with 19 chapters covering the most important topics in onco-nephrology that can be accessed here: https://www.asn-online.org/education/distancelearning/curricula/onco/.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.