The patient is a 64-year-old female who presents with 4.5 grams of proteinuria, hematuria, and a creatinine of 1.5. She has a history of hypertension and coronary artery disease.
What is the best diagnosis?
A. Arterionephrosclerosis
B. Focal Segmental Glomerulosclerosis
C. Amyloidosis
D. Fibrillary Glomerulonephritis
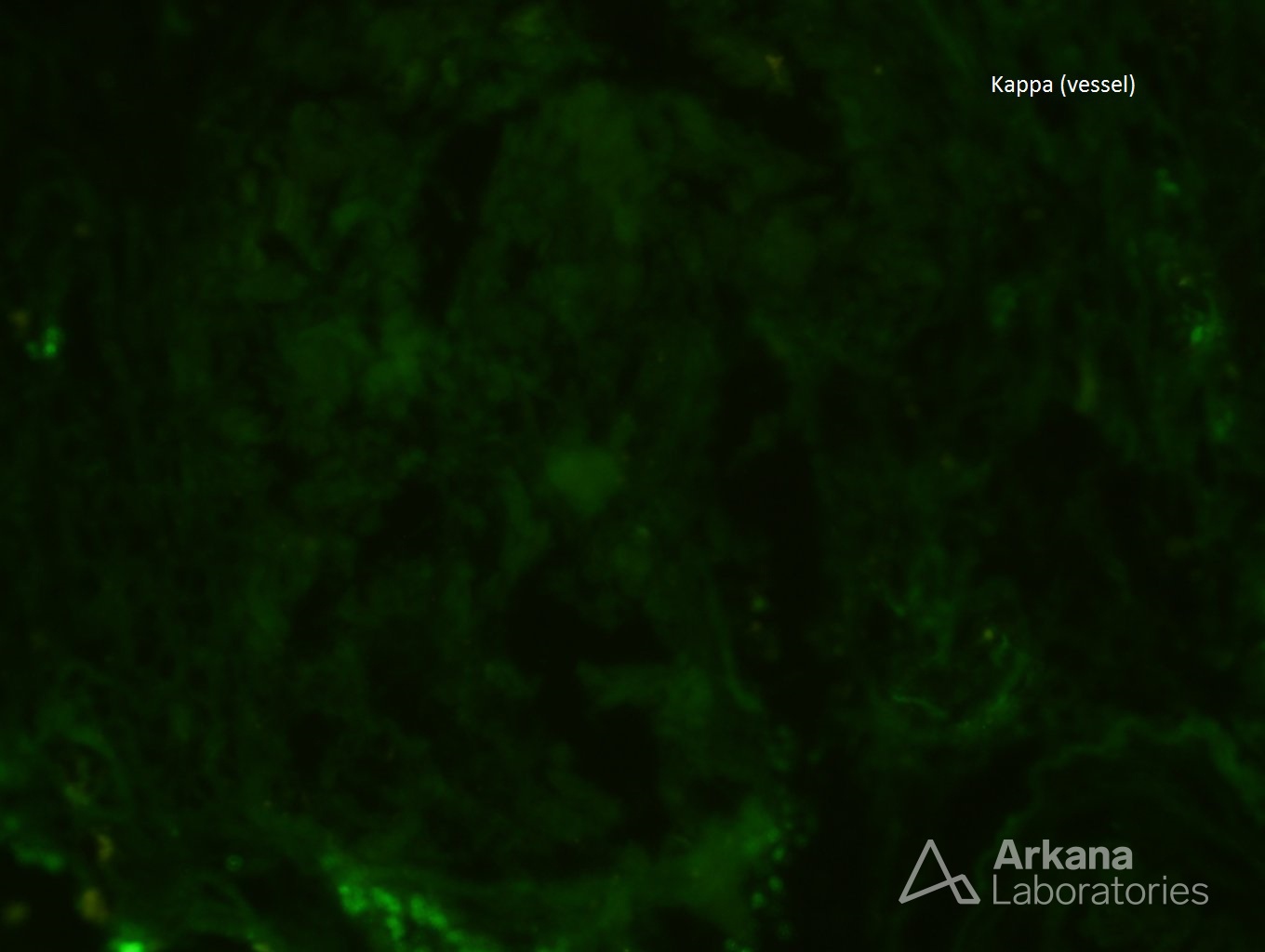
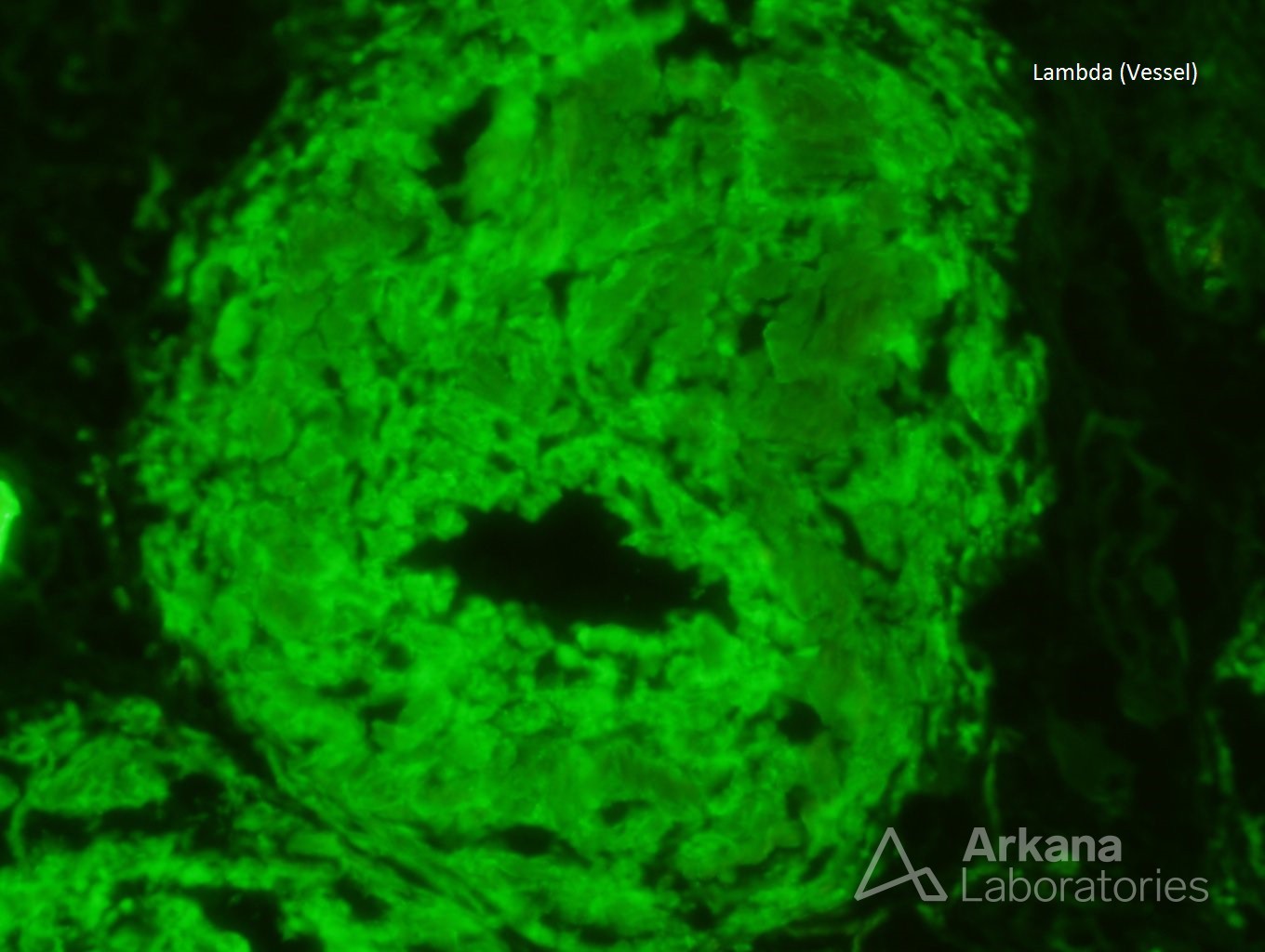
The best answer is C: Amyloidosis.
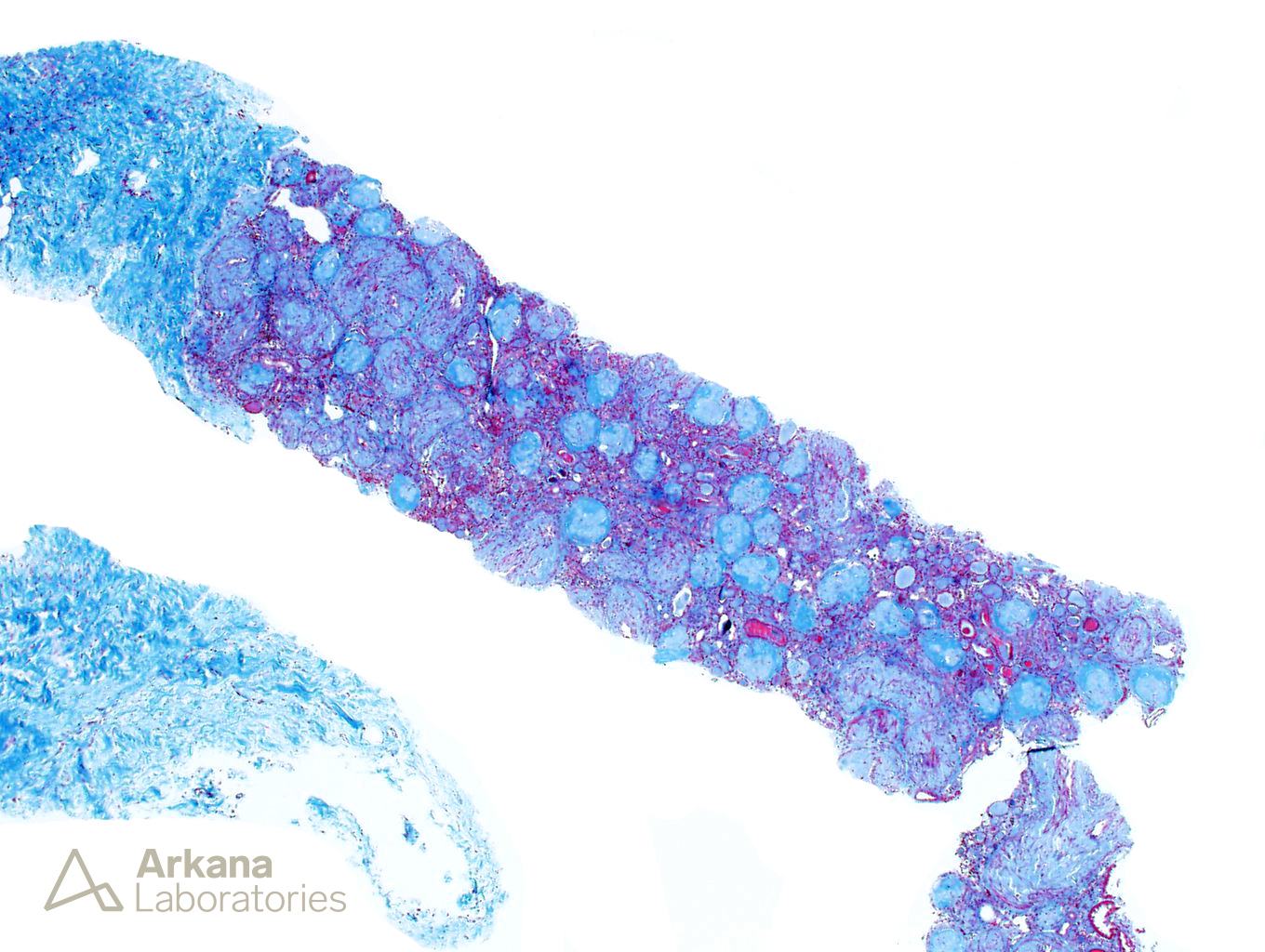
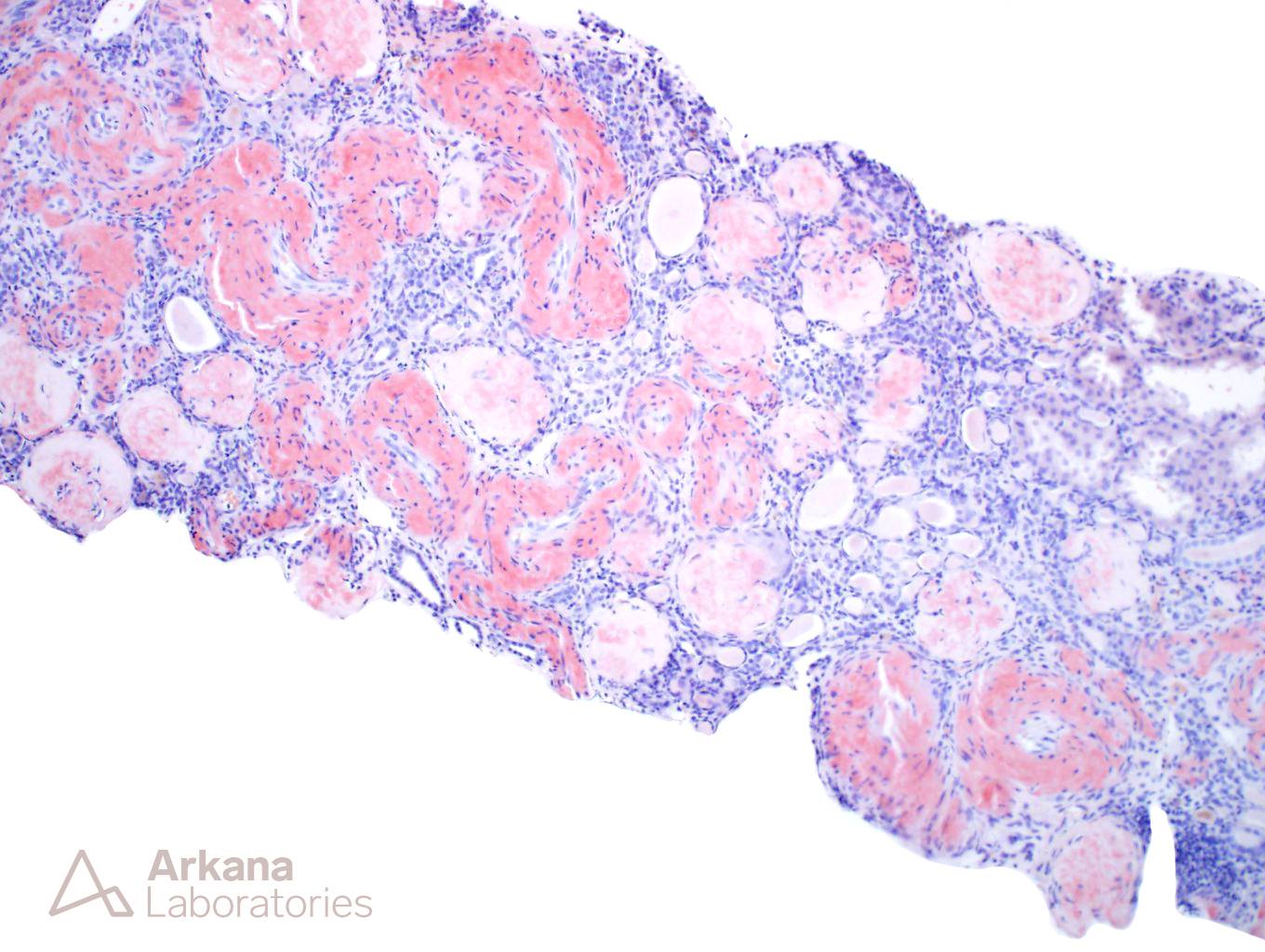
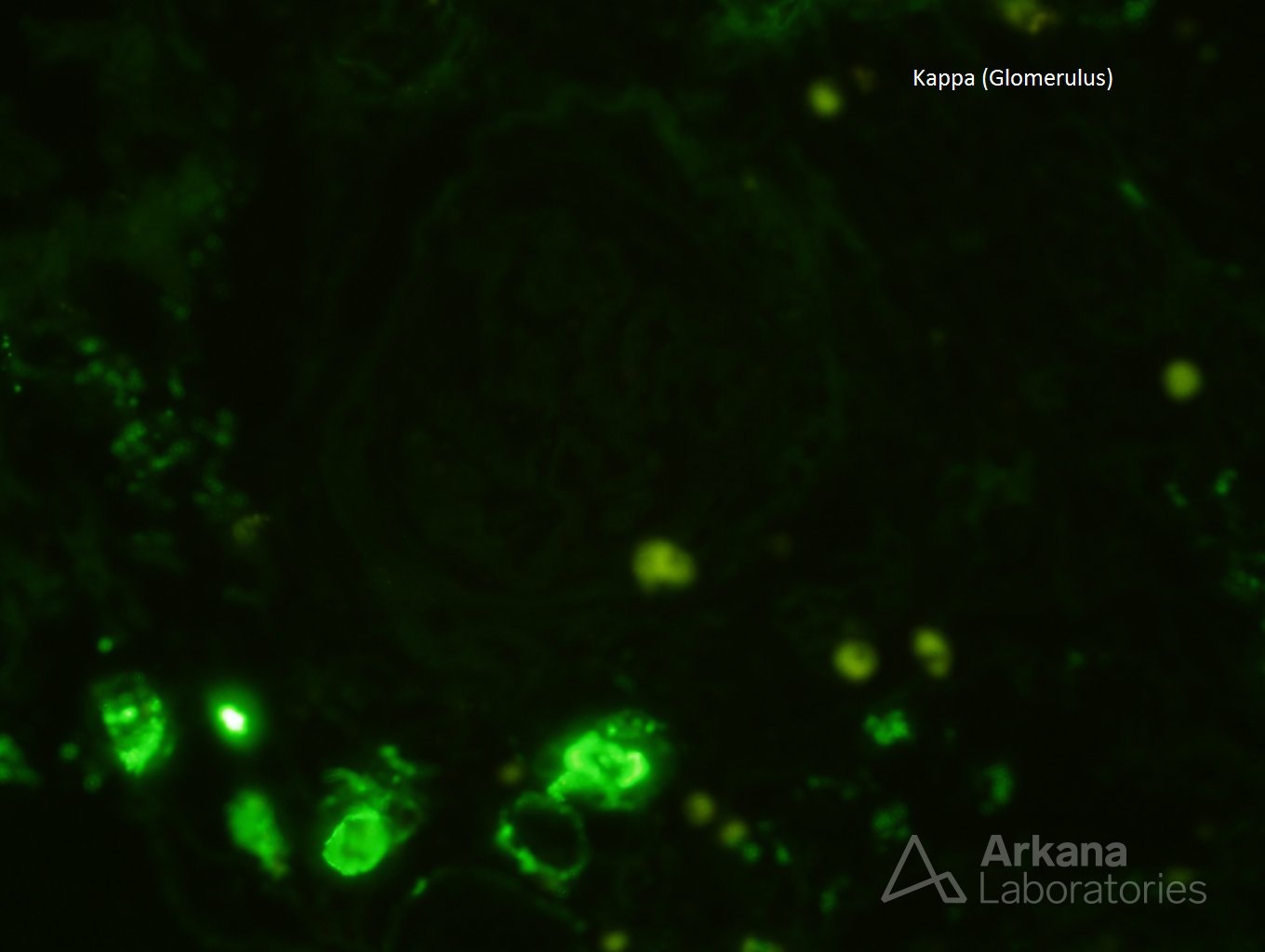
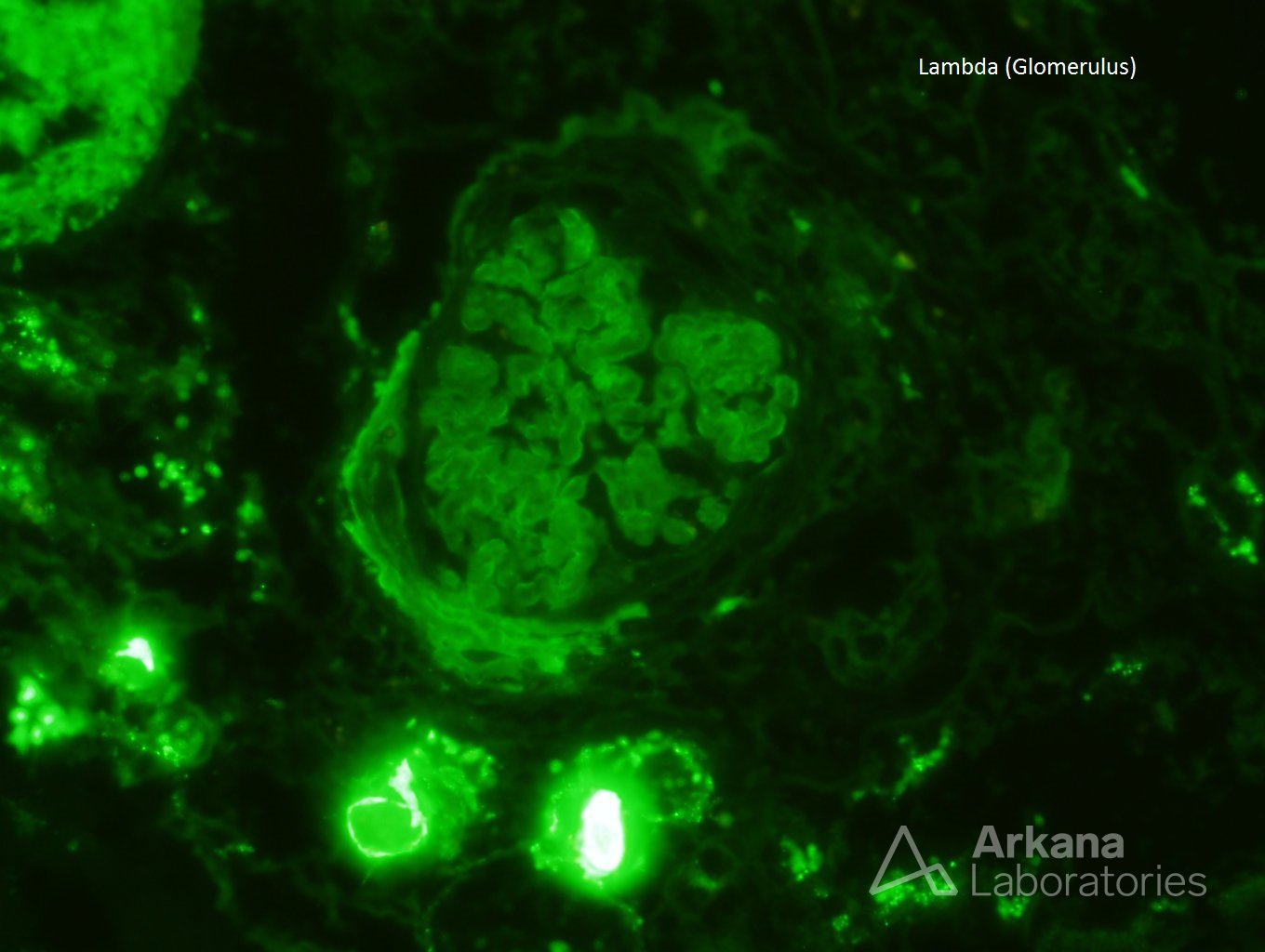
The biopsy, at first glance, looks like a subcapsular scar with diffuse global glomerulosclerosis. In this setting, arterionephrosclerosis would provide a good explanation for this distribution of fibrosis especially with the severe arteriosclerosis seen in the vessel. FSGS is also a consideration and can produce segmental scars with extensive global glomerulosclerosis. However, the presence of Congo red positivity and lambda light chain restriction within the glomeruli and vessels is diagnostic for amyloidosis, AL type. Fibrillary glomerulonephritis would not affect the vessels and is Congo red negative.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.