The presence of two APOL1 risk alleles, which predominantly affect populations of recent African ancestry, confers up to 29x increased risk for renal disease. The morphologic manifestation of APOL1-mediated kidney disease is quite variable, and includes focal segmental glomerulosclerosis (FSGS), collapsing glomerulopathy, and non-specific glomerular and tubulointerstitial arterionephrosclerosis-like chronic changes (see reference).
To develop renal disease, carriers of two APOL1 risk alleles are believed to require either additional genetic alterations that contribute to the disease or additional environmental risk factors. Some of these known factors include HIV infection, COVID-19, sickle cell disease, systemic lupus erythematosus, and membranous glomerulopathy, among others. The biopsy shown is from a 25-year-old African American patient who presented with hematuria, proteinuria, and chronic kidney disease.
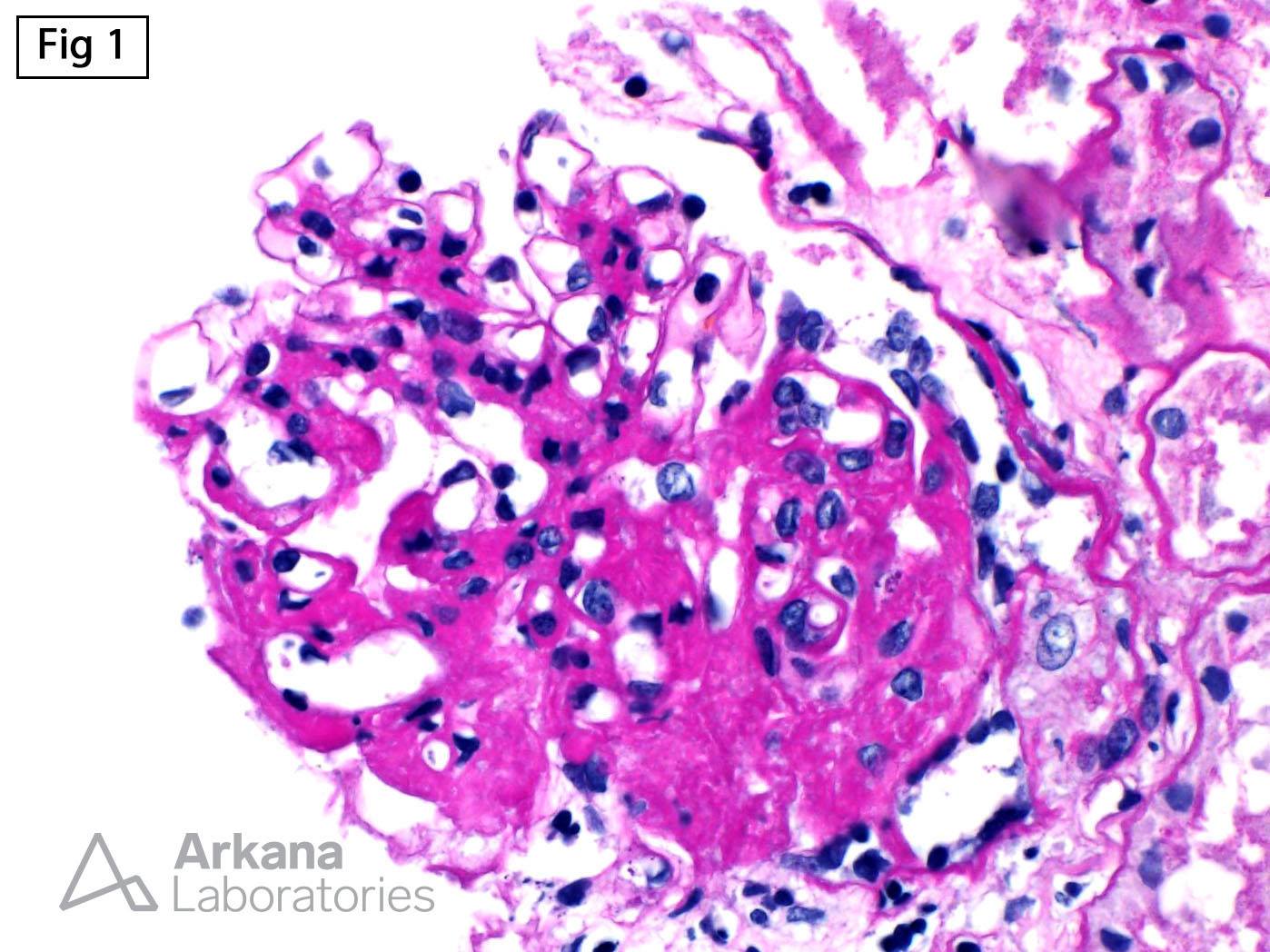
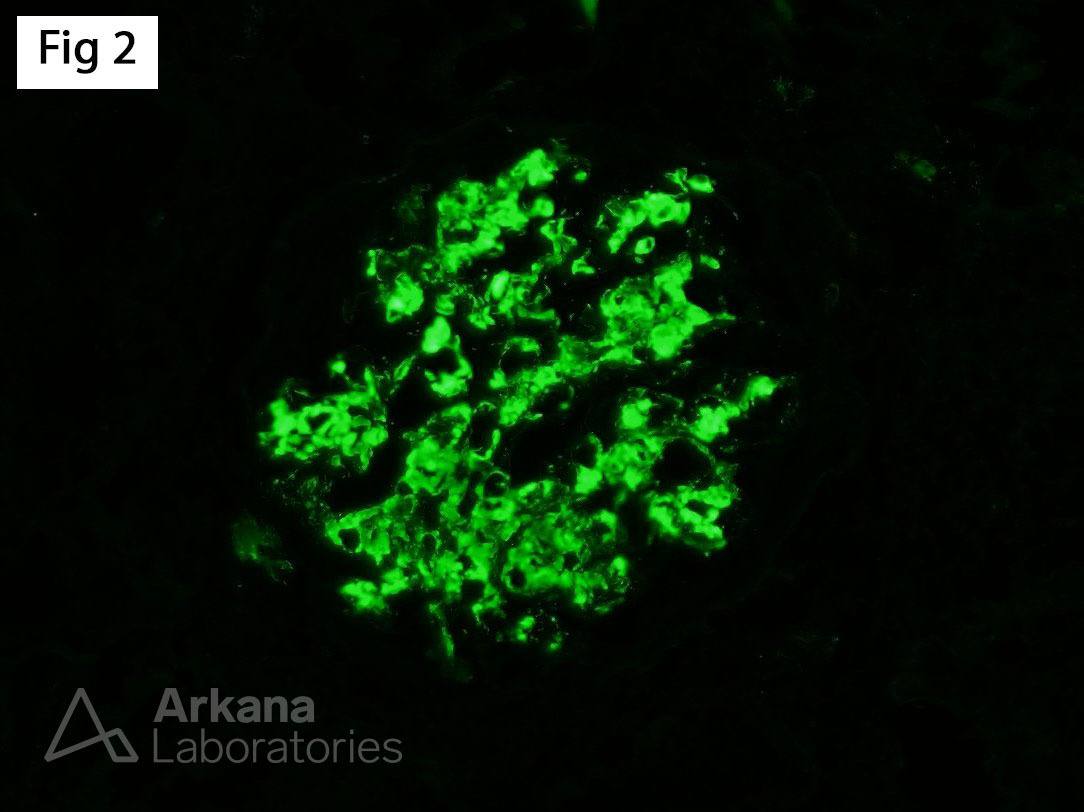
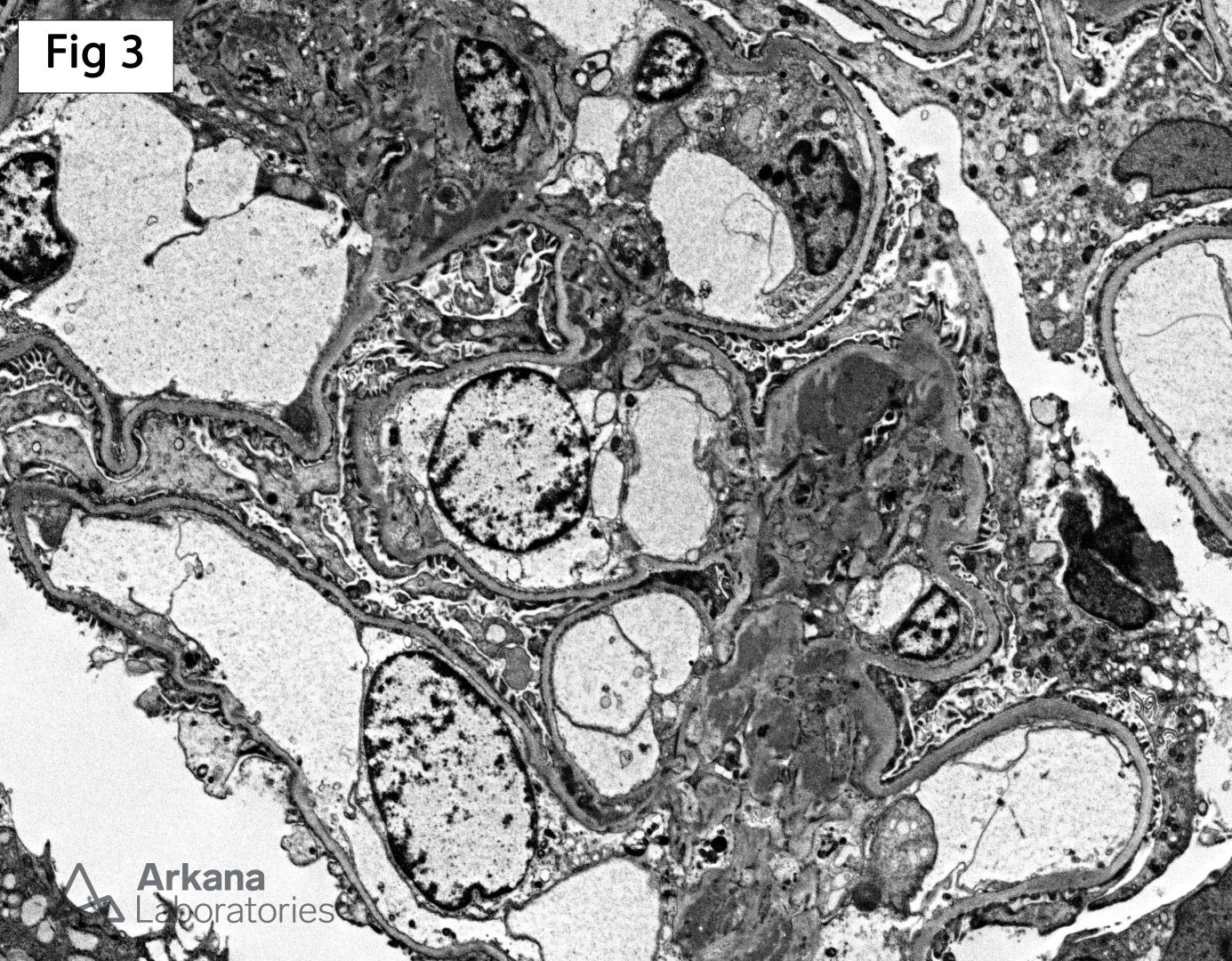
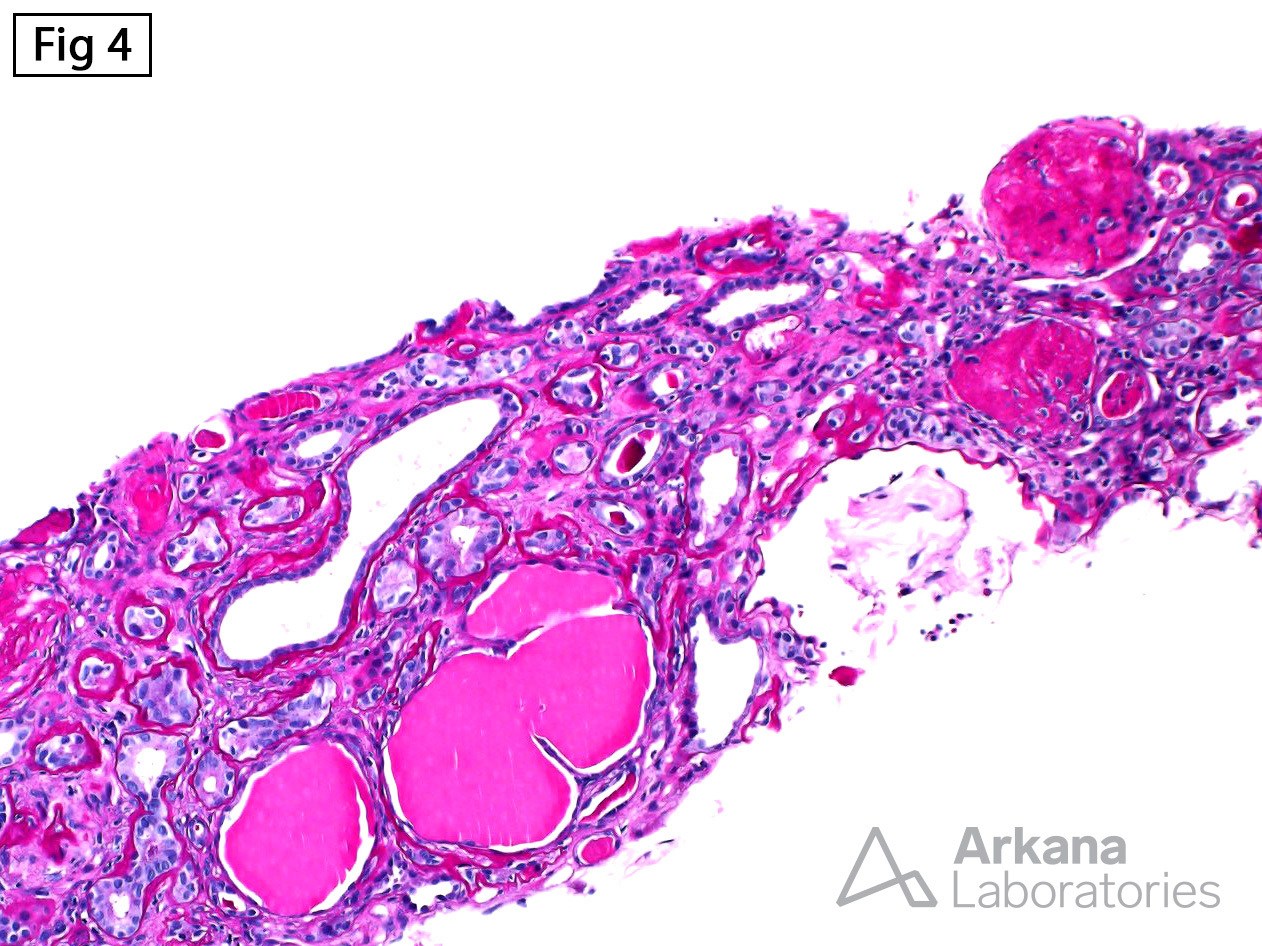
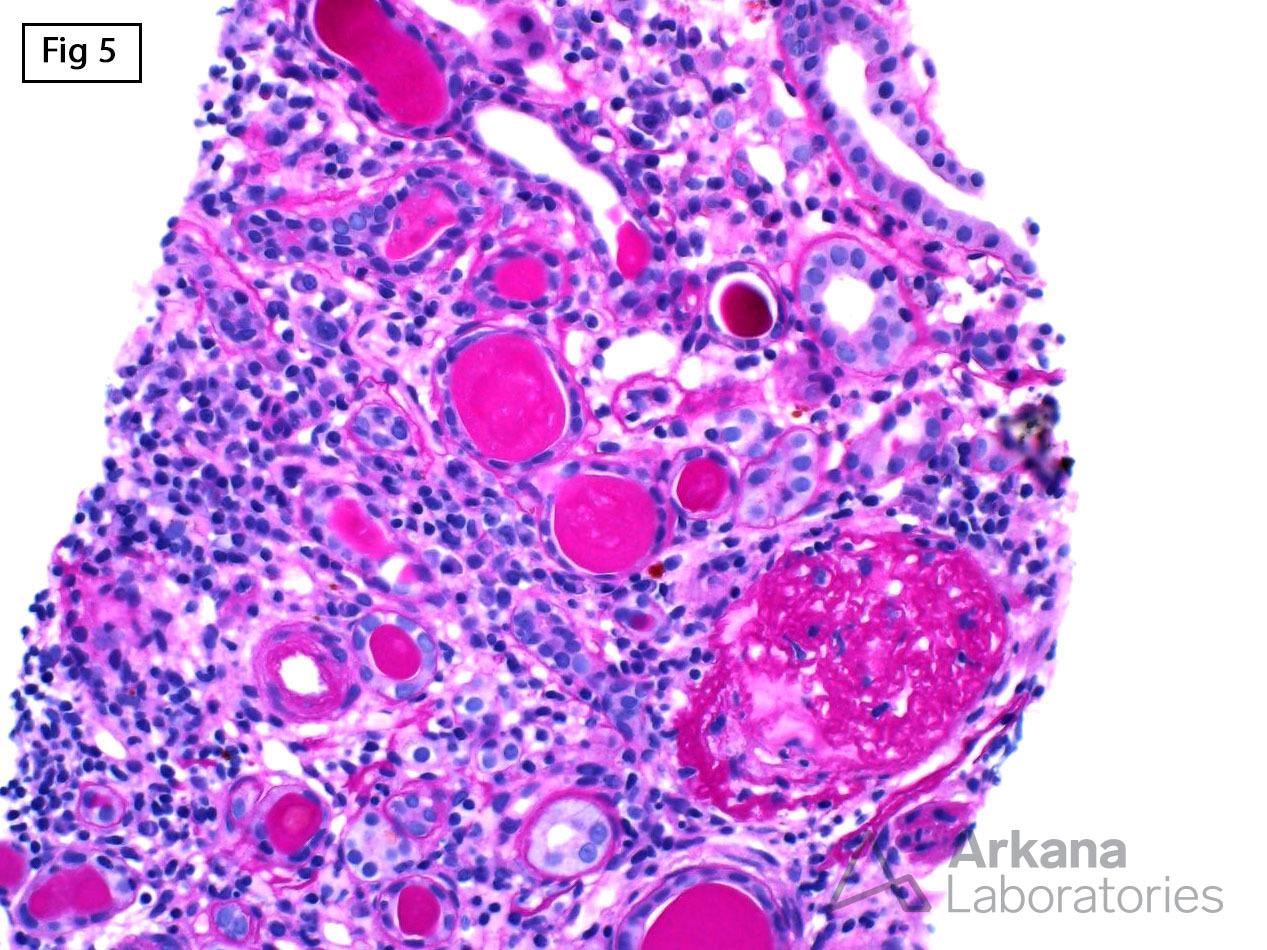
The morphologic changes are diagnostic of IgA nephropathy (Figures 1, 2 and 3). However, the biopsy also showed frequent disappearing and solidified-type globally sclerotic glomeruli along with early microcystic tubular dilatation (Fig 4 and 5). Subsequent genetic testing showed the presence of two APOL1 risk alleles which is indicative of concurrent IgA and APOL1-mediated kidney disease.
Reference: Larsen CP, Beggs ML, Saeed M, et al. Histopathologic findings associated with APOL1 risk variants in chronic kidney disease. Mod Pathol 2015; 28: 95-102
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.